In this material Multimodal Monitoring in ICU's is described in this aspects:
- Description of commonly used invasive multimodality monitoring techniques
- Indications, patient selection, and safety of multimodality monitoring
- Current evidence on how multimodality monitoring can guide treatment in
specific patient populations
KEY POINTS
I n patients with severe acute brain injury, the neurologic examination is often
insensitive to detect neurological deterioration, and traditional physiological
assessments such as heart rate, oxygen saturation, and blood pressure lack
sensitivity and specifi city for detecting changes in neuronal function.
● The use of invasive cerebral monitoring tools to supplement the neurological
exam is a rapidly evolving approach in clinical practice despite limited
high-quality evidence to guide their use.
● Multimodality monitoring (MMM) utilizes either direct measurements or surrogates
to assess intracranial pressure (ICP), cerebral autoregulation, brain
temperature, oxygenation, and metabolism. These fi ndings can help guide
medical and surgical interventions, monitor responses to treatment, and aid
in neuroprognostication.
● MMM can detect secondary brain injury in “real time”; however, more widespread
implementation is limited by the complexities of data visualization
and analysis.
● The International Multidisciplinary Consensus Conference on Multimodality
Monitoring in Neurocritical Care derived a summary statement with recommendations for the use of such tools based on available data. Similarly,
the International Microdialysis Forum released a consensus statement summarizing
the evidence and providing guidance for the use of cerebral metabolism
markers in neurocritically ill patients.
Traditional assessment in critically ill comatose patients
Clinical examination is often limited in patients with severe acute brain injury and
may be insuffi cient to detect secondary brain injury, which is intimately related to
outcomes and may respond to time-sensitive interventions.
● Cardiopulmonary complications are common after acute brain injury and can impact the clinical course and outcomes of neurocritically ill patients. Systemic hemodynamic monitoring leads to better understanding of the pathophysiology of circulatory failure while providing qualitative and quantitative measures of insufficientorgan perfusion.
● Routine physiologic monitoring such as invasive continuous blood pressure, heart
rate, and pulse oximetry are typically employed in all critically ill patients.
● I n patients with evidence of myocardial dysfunction or hemodynamic instability, cardiac
output, echocardiography, and intravascular volume assessments should be
considered. Nevertheless, these tools lack sensitivity and specifi city for detection
of neuronal injury.
● I maging studies are crucial in the evaluation of neurocritically ill patients but have
limited temporal resolution and are not benign given the potential risks associated
with transporting patients outside the ICU.
● Continuous EEG (cEEG) is noninvasive and allows continuous monitoring, but has
limited spatial resolution and is labor intensive.
Uses and indications of invasive multimodality monitoring
Multimodality monitoring (MMM) allows assessment of multiple physiological
parameters.
● Primary goals for MMM include the following:
Detect early neurologic deterioration that may benefi t from time-sensitive interventions to prevent irreversible damage.
Guide patient management by individualizing patient care decisions.
Monitor responses to treatment and tailor subsequent therapeutic decisions to
avoid adverse effects.
Enhance the understanding of pathophysiology and disease processes that
lead to secondary brain injury, and advance the fi eld by developing potential
therapies targeting specifi c disease mechanisms.
● MMM technology is most applicable to neurocritically ill patients with poor-grade
subarachnoid hemorrhage (SAH), intracerebral hemorrhage (ICH), and severe traumatic brain injury (TBI).
● MMM may also help management of patients with large vessel acute ischemic
strokes (AIS), cardiac arrest (CA), and selected cases of refractory status epilepticus.
Limitations and complications of MMM
Choice of the mode of monitoring, region of interest, and placement remains debatable
and should be tailored to the specifi c clinical question and primary pathologic
process.
Many practitioners place probes in at-risk or penumbral tissue, for example, the
vascular territory felt most likely to be affected by vasospasm after SAH, or the
vascular territory most at risk of herniation in the setting of large AIS.
Invasive monitoring is also commonly performed in areas of relatively normal
brain tissue.
However, monitoring contralateral to the injury may be of limited value, and
monitoring in the center of the pathology (i.e., inside a blood clot) is of no value.
Some commercially available devices allow for concurrent monitoring of three
parameters with a single probe: parenchymal intracranial pressure (ICP), brain
temperature, and PbtO2.
Widespread implementation of MMM is limited by lack of integrated software
that allows for easy analysis and interpretation in real time at the bedside.
● The safety profi le of the majority of tools commonly used in MMM is excellent; however, potential complications include focal hemorrhage (immediate 2%, delayed
1%) and ventriculitis (4%–5%, depending on whether the patient has concurrent
ventriculostomy).
Evidence to support widespread use of MMM is limited:
MMM has failed to show consistent impact on outcomes: The physiologic
information obtained may translate into benefi ts in a selected group of patients
but not others, thus leading to a dilution of the overall benefi t.
There is a paucity of randomized clinical trials evaluating the utility of MMM:
Anecdoetal evidence of benefi t (e.g., ICP monitors in selected patients) has led
to lack of equipoise and reluctance to withhold potentially life-saving monitoring
that would be required in a traditional randomized trial.
The development of treatment algorithms derived from the information obtained
from MMM is still in its relative infancy.
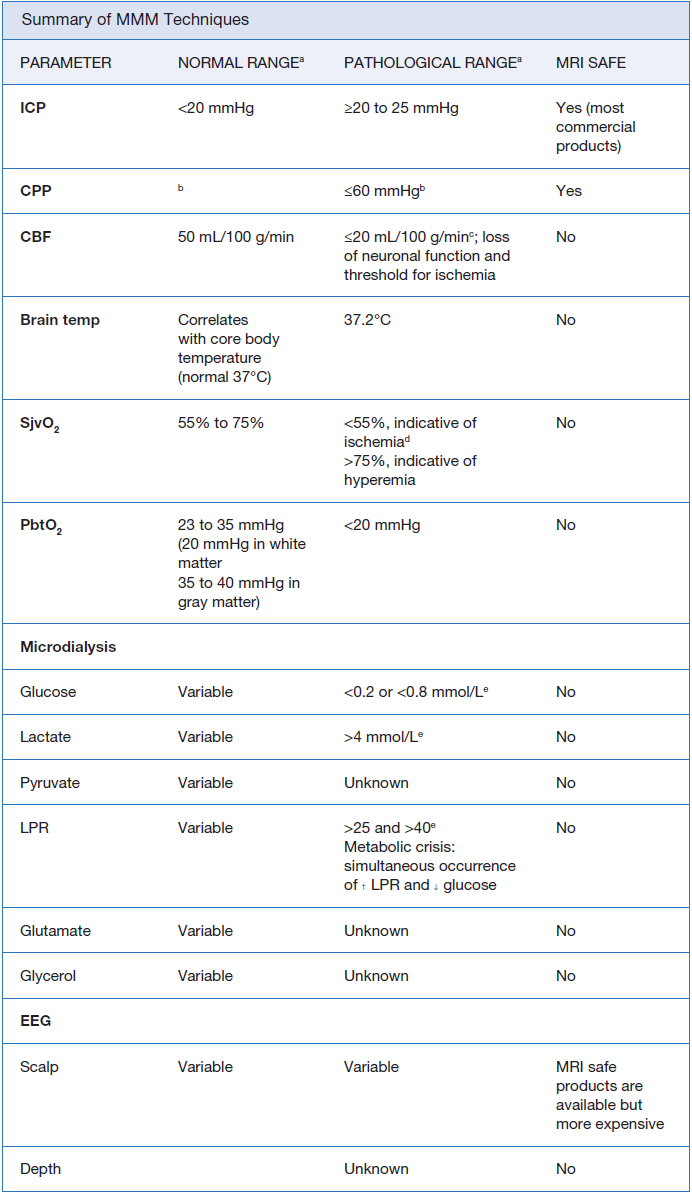
Basics of MMM
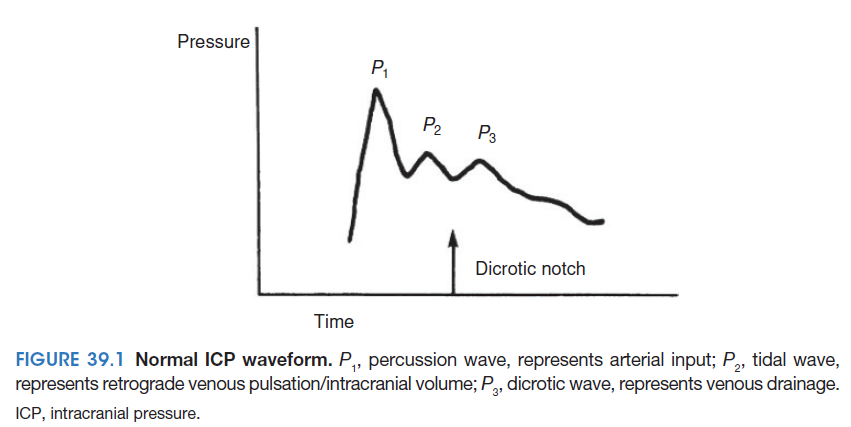
- Intracranial pressure. I CP is the most commonly measured parameter in neurocritical care units. I CP is measured in millimeters of mercury (mmHg) via an intracranial device inserted into one of the following locations: subdural, epidural, parenchymal, or ventricular.
- Brain oxygenation. Inadequate systemic and brain oxygenation exacerbates secondary brain injury. Brain oxygen monitoring should be considered in all patients at risk of cerebral ischemia and/or hypoxia. There are various means of assessing brain oxygenation: partial brain tissue oxygen tension (PbtO2), jugular bulb venous saturation (SjvO2), and near-infrared spectroscopy (NIRS).
- Microdialysis. Microdialysis (MD) involves invasive measurement of the concentration of metabolites and cell breakdown products in brain tissue extracellular fl uid. MD may also be used to remove potentially detrimental large molecules such as infl ammatory mediators using catheters with a 100-kDa membrane. Such catheters are available but not U.S. Food and Drug Administration (FDA) approved yet. Measuring probes are typically placed in the subcortical region of interest via tunneling technique (often during craniotomies for another indication) or via burr hole with a bolt placed at bedside. MD data is a regional measure reflecting 2 to 3 mm of brain tissue surrounding the probe. Safety profi le is excellent, but data is limited to a small fi eld of view and the technique is time consuming, providing relatively delayed data (within 60 minutes).
- Cerebral blood flow. CBF is a critical variable for brain function and may be helpful in identifying ischemic thresholds when coupled with measurements of metabolic demand. Imaging studies such as CT or magnetic resonance perfusion can estimate CBF at one point in time, but have very poor temporal resolution and are diffi cult to repeat serially. Obtaining continuous CBF measures is challenging, but indirect estimates of perfusion can be made with invasive techniques. Measurement of CBF is accomplished by placing a probe into brain parenchyma
through a burr hole. The use of such probes is limited by its small fi eld of view and the optimal location of placement is debatable. - Brain temperature. The incidence of hyperthermia is high in acute brain injury patients and may be a marker for poor outcome. Temperature modulation may decrease bioenergetic failure (diagnosed by MD) and assist in controlling ICP. Core temperature is a reasonable surrogate for brain temperature as brain-to-core
temperature ratio is quite predictable and constant, even in acute brain injury. Direct brain temperature can be measured via a thermocouple probe inserted into
brain parenchyma through a burr hole, often in conjunction with other invasive monitoring measures including ICP and PbtO2. At this time, brain temperature measurements are a research tool. - Intracortical electroencephalography (or “depth” electrode). Highly epileptogenic patterns or seizures detected through intracortical electroencephalography (ICE) may be invisible to scalp EEG. I n addition, nonseizure-related secondary neurological injury may exhibit early ICEspecifi
c signatures detected hours before other monitoring modalities. I t is used in conjunction with scalp cEEG monitoring. I deal placement is determined on a case-by-case basis with the goal of placing the electrode into brain tissue at maximal risk of secondary injury. However, the clinical significance of EEG findings seen on depth electrodes that are not visualized on scalp EEG remains uncertain.
FUTURE CONSIDERATIONS/REMAINING QUESTIONS/CHALLENGES
- MMM utilization and promises. Although MMM is in use at several medical centers in the United States and Europe, it is not part of routine clinical care of neurologically critically ill patients at most centers. Recent guidelines summarizing the evidence in favor of safety profi le, prognostic value, and providing more homogenous recommendations regarding their indications may boost the widespread use of these tools. Normal values for the metabolites have been established to help guide clinicians in interpreting this data; however, variations over time and changes in response to therapeutic interventions may be more useful. Ultimately, whether these thresholds represent outcome-modifying targets is still unproven. The interpretation of values for each parameter should take into consideration the values of other available multimodal monitoring parameters, the specific primary disease process, the stage of the clinical course, and whether or not therapeutic interventions were implemented.
- Impact of MMM on outcome. Knowledge of relationship of MMM parameters and outcome is in its infancy. Answers depend both on performance of devices as well as the therapeutic intervention and the timing of its implementation.
- Large multicenter prospective trials are needed. Results could drive algorithmic approaches to physiologic, metabolic, and electrical consequences of acute brain injury. Lacking such trials, each patient for whom MMM is employed should be treated on a case-by-case basis.
- Major goals for the future. Development of automated alarm systems that are sensitive and specific enough to identify secondary injury when permanent damage can still be prevented. Combining MMM with other techniques, including proteomics or imaging, may offer further insights into mechanisms underlying acute brain injury. The future of MMM lies in the ability to visualize and computationally analyze patient-specifi c “physiologic profi les” that can be trended over time and used in “real time” to anticipate, treat, and ideally prevent further insults in the unresponsive, acutely brain-injured patients.
Cases
References
1. Le Roux P, Menon DK, Citerio G, et al. Consensus summary statement of the International Multidisciplinary Consensus Conference on Multimodality monitoring in neurocritical care: a statement for healthcare professionals from the Neurocritical Care Society and the European Society of Intensive Care Medicine. Neurocrit Care. 2014;21(Suppl 2):S1–S26.
2. Hutchinson PJ, Jalloh I, Helmy A, et al. Consensus statement from the 2014 International Microdialysis Forum. Intensive Care Med. 2015;41(9):1517–1528.
3. Stuart RM, Schmidt M, Kurtz P, et al. Intracranial multimodal monitoring for acute brain injury: a single institution review of current practices. Neurocrit Care. 2010;12(2):188–198.
4. Hutchinson PJ, O’Phelan K. International multidisciplinary consensus conference on
multimodality monitoring: cerebral metabolism. Neurocrit Care. 2014;21(Suppl 2):S148–S158.
5. Stein NR, McArthur DL, Etchepare M, et al. Early cerebral metabolic crisis after TBI infl uences outcome despite adequate hemodynamic resuscitation. Neurocrit Care. 2012;1:49–57.
6. Carney N, Totten AM, O’Reilly C, et al. Guidelines for the management of severe traumatic brain injury, Fourth Edition. Neurosurgery. 2017;80(1):6–15.
7. Reinstrup P, Stahl N, Mellergard P, et al. Intracerebral microdialysis in clinical practice: baseline values for chemical markers during wakefulness, anesthesia, and neurosurgery. Neurosurgery. 2000;47(3):701–709; discussion 709–710.
8. Schmidt JM, Ko SB, Helbok R, et al. Cerebral perfusion pressure thresholds for brain tissue hypoxia and metabolic crisis after poor-grade subarachnoid hemorrhage. Stroke. 2011;42(5):1351–1356.
9. Tisdall MM, Smith M. Cerebral microdialysis: research technique or clinical tool. Br J Anaesth. 2006;97(1):18–25.
10. Barth M, Woitzik J, Weiss C, et al. Correlation of clinical outcome with pressure-, oxygen-, and fl ow-related indices of cerebrovascular reactivity in patients following aneurysmal SAH. Neurocrit Care. 2010;12(2):234–243.
11. Waziri A, Claassen J, Stuart RM, et al. Intracortical electroencephalography in acute brain injury. Ann Neurol. 2009;66(3):366–377.
12. Stuart RM, Waziri A, Weintraub D, et al. Intracortical EEG for the detection of vasospasm in patients with poor-grade subarachnoid hemorrhage. Neurocrit Care. 2010;13(3):355–358.