The problem description
EEG method now widely used for epilepsy diagnosis, but EEG is not specific enough, it means that if patient has no epileptiform activity on EEG, it does not mean that he has no epilepsy. And if the patient has epileptiform activity on EEG, it does not mean that he has epilepsy.
Some times we ca define some EEG patterns, which are look like spikes or sharp waves, but this abnormalities are not epilepticus.
Epileptiform activity on EEG
Before we go to non epilepticus EEG pattern, lets overview of some epileptic patterns:
Epileptiformactivity on EEG can be provoked with activation tests:
- Photic stimulation (from 1 up to 60 Hz).
- Hyperventilation.
- Falling asleep (sleep deprivation is needed).
Overview of some non epilepticalpatterns on EEG
Lambda-waves
Lambda-waves are the positive sharp waves, located in occipital EEG derivations with frequency 4-5 Hz during awake while solving some visual tasks.
•Located in the occipital regions bilaterally as positive waves.
•Triangular in shape (like the capital lambda: Λ) and generally symmetric.
•Amplitude: 50 mV
•Duration 200-300 msec
•Present with eyes opened and during visual fixation
•Same morphology as POSTS (Positive occipital sharp transients of sleep), both in form and in occipital distribution, however POSTS are during sleep.
Positive Occipital Sharp Transients of Sleep, POSTS
POSTS are the positive sharp waves, looked similar to Lambda waves, and normal for 50-80% of healthy people during NREM-sleep. Quite frequently this waves are registered on children and young people during falling a sleep.
•Located in the occipital regions bilaterally as positive waves, during drowsiness/sleep
•Triangular in shape (like the capital lambda: Λ, only upside down) and generally symmetric.
•Most evident in non-REM 1 and non-REM 2
•Same morphology as Lambda waves, both in form and in occipital distribution, however lambda waves are during awake state, when visually fixating.
•POSTS are completely normal, should not be confused with spikes
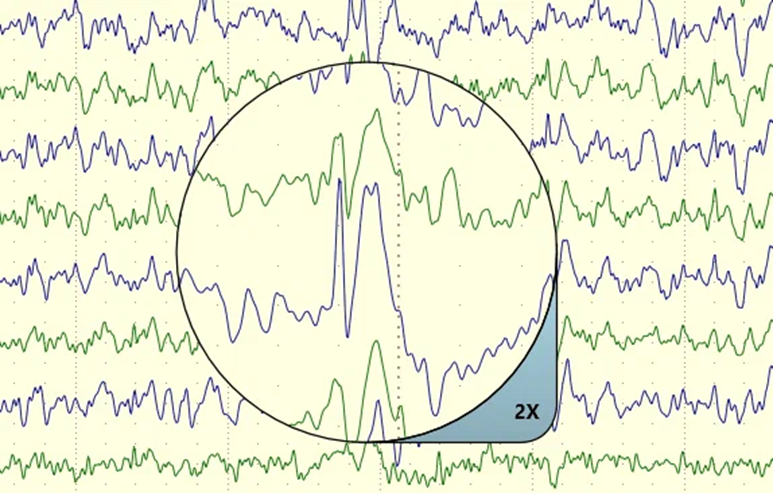
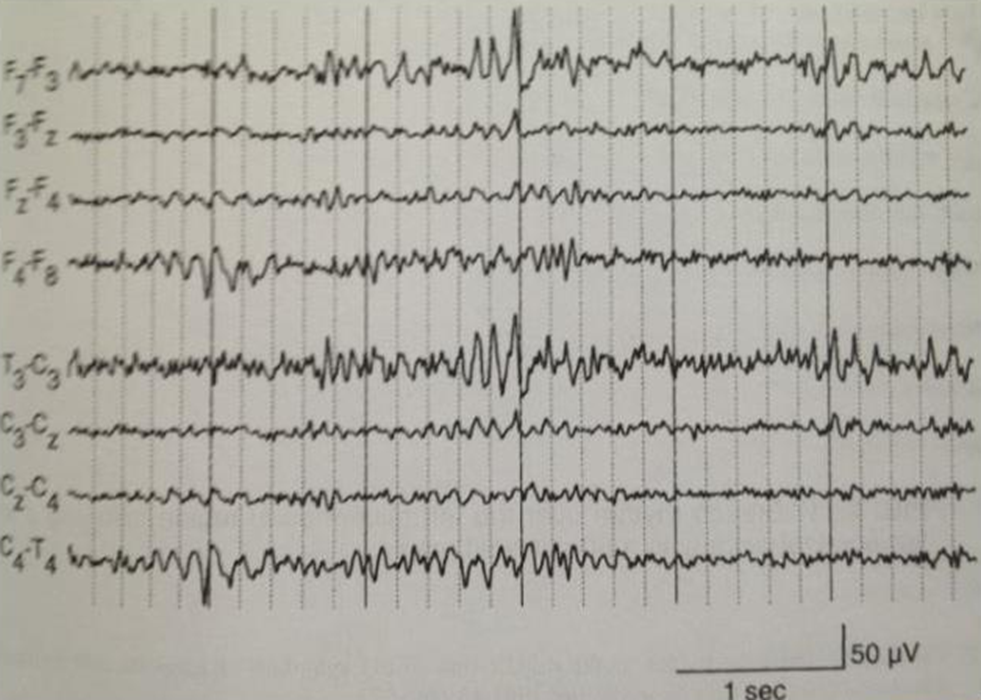
Phantom 6 Hz spikes
It is a tiny low amplitude spikes, some times spike + slow wave complex. Usually they have 5-6 Hz frequency and amplitude less then 40 mA. Duration usually less then 30 ms. This wave are normal for children and young people in frontal and occipital areas.
•6 Hz spike-and-wave bursts (WHAM and FOLD)
•Synonymes: Phantom spike and waves
•Brief bursts of low amplitude spike-and-slow wave 6Hz (5-7Hz)
•Spike often not clearly discernible: “phantom”
•Bilateral and synchronous
•Maximal at midline (posterior or anterior)
•Relaxed wakefulness and drowsiness
•Adolescents and young adults
•duration of 1-2 seconds
Two subtypes of 6 Hz spike-and-wave bursts
•WHAM: Waking, High amplitude spike (>45uV), Anterior, Male
•Associated with epilepsy especially when high amplitude spikes,
rate <5-6Hz and persists during deep sleep
•FOLD: Female, Occipital, Low amplitude spike, Drowsy
•Not associated with epilepsy
Positive 14 and 6 Hz spikes (Ctenoids)
Located in occipital area during awake or N1 sleep stage.
14 & 6 Hz positive bursts:
- Synonymes: ctenoids
- Bursts of 14Hz (13-17) or 6Hz (5-7)
- Duration: 0.5-1 second
- Unilateral (R>L) or bilateral asynchronous or synchronous
- Arch-shaped waves / Positive sharp peaks
- Maximum in posterior temporal region
- Present in drowsiness and light sleep
- Young adults
- Not associated with epilepsy
Vertex sharp potential, VSP
One or two phasic wave (same time three phasic wave), located in vertex and central area. Duration is about 100 ms. Normal for NREM-sleep.
- Synonymes: Vertex sharp transient or V wave:
- Amplitude: 50-150 microV
- Narrower and more focal than K complex
- In children and young adult vertex waves could be sharp and in a repetitive run, not to be confused with an epileptic discharge.
K-complex
Monophasic waves with duration 0.5 sec frequently goes with vertex waves on central derivations during sleep stage 2.
Benign Epileptiform Transients of Sleep, BETS
Small Sharp Spikes – monophasic or two phasic waves with small amplitude during N1 and N2 sleep stages. Amplitude is usually less then 90 ms. They are normal for adults. Located in middle lobe and temporal areas.
Small sharp spikes (SSS) Synonymes: BETS (Benign EpileptiformTransients of Sleep) and benign sporadic sleep spikes:
- Occur in light sleep (non-REM 1 and 2 sleep)
- Amplitude of <50 microV and duration of <50 ms
- Usually monophasic, occasionally diphasic
- Occasionally followed by a slow wave, however do not disturb the background
- Located temporal uni- or bilateral
- Incidence of 20%
- Small sharp spikes are not associated with epilepsy
Wicket Waves, Wicket Rhythm
PolyphasicEEG-pattern 7-12 Hz with symmetries growing and decreasing amplitude. Normal in awake state.
Wicket spikes:
- Short runs of 6-11Hz spikes, sometimes single spike
- usually within alpha frequency range
- Monophasic arciform waveforms (60-200uV)
- Anterior or mid-temporal region
- Usually present unilaterally with shifting emphasis between sides
- Sharp monophasic, no slow wave
- Present in relaxed wakefulness, drowsiness, light sleep
- Usually in middle and late adulthood
- Clinical significance: analogue of the auditory alpha rhythm
- May decrease with auditory stimulation
- Not associated with epilepsy
Rhythmic Mid-temporal Theta of Drowsiness, RMTD
Theta waves during awaking and drowsing. Located in middle temporal area.
Synonymes: Rhythmic midtemporaldischarges, RTTD, psychomotor variant pattern:
•Trains of rhythmic theta waves 5-7Hz
•Duration 5-10sec
•Located in midtemporalregion
•Often unilateral
•May be bisynchronous, with shifting asymmetry between sides
•Present in relaxed wakefulness and drowsiness
•Adolescents and adults
•Does not change in frequency or form, in contrast to an epileptic discharge.
•Not associated with epilepsy
Subclinical Rhythmic Electroencephalographic Discharges of Adults, SREDA
From delta to theta rhythmic activity during N1 sleep stage or awaking. Some times it can be activated by Hypoventilation. Located mostly in temporal and lobe areas, usually symmetric. Duration of episodes can be from 10 sec up to 5 min.
SREDA (Subclinical rhythmic electrographic discharge in adults)
•Abrupt onset and termination of sharp rhythmic theta rhythm of 5-7Hz
•Constant frequency
•Duration of 40-80 sec
•Located Parietal and Posterior temporal
•Bilateral and synchronous, symmetrical (however sometimes unilateral)
•No change in localization of frequency
•Present in wakefulness, drowsiness, stage II sleep
•Trigger: Hyperventilation
•Usually in people >50 years
•Uncommon (incidence <0.05%)
•Not associated with epilepsy
Conclusion
To define EEG patterns correctly, pay attention to:
- Sleep / awake / drowsiness condition
- Morphology of the pattern
- Amplitude of waves
- Localization of pattern
- Patient age and sex
References
8. EEGPedia.