НЕ ДЛЯ ПЕЧАТИ
Khidirbegishvili O.E. Dentist. Tbilisi, Georgia
Abstract.For many years it has not been possible to finally resolve the issue of attributing the progressive forms of carious lesions localized on the pulp chamber vault to caries or pulpitis. In some countries this pathology is attributed to carious lesions, and in others to pulp lesions. In addition, in the treatment of such lesions, the question of selective and non-selective method of removal of softened parapulpal dentin has not yet been unequivocally resolved. This article is devoted to this issue of modern dentistry.
Keywords: progressive dentin caries, initial pulpitis, reversible, irreversible pulpitis, traumatic pulpitis, pulp hyperemia, pulp atrophy.
INTRODUCTION
One of the priority areas of clinical dentistry the introduction of minimally invasive techniques for maintaining pulp viability. However, the question has not yet been definitively resolved – which method of removing demineralized dentin (selective or non-selective) is preferable to use in the biological treatment of inflamed pulp. In addition, it is unclear to which disease (caries or initial pulpitis) progressive carious pathology should be attributed, localized in the vault of the pulp chamber, for the treatment of which a biological method of treating inflamed pulp is used.
For example, in Russia it is referred to as acute deep caries The American Dental Association (ADA) attributes this pathology to caries, which spreads to the pulp cavity and even to the root canal system.The European Endodontic Society (ESE) considers this pathology to be very deep caries ( extremely deep caries). In my proposed classification of caries, this nosology is diagnosed as «progressive dentine caries».Despite this, the WHO defiantly considers it an initial pulpitis for some reason.Even more surprising, when in the WHO classification of pulpitis, the initial pulpitis includes diseases that differ in clinical and morphological data, for the treatment of which completely different methods are used (direct and indirect capping of the pulp).
Unambiguously, the nosology of "initial pulpitis", in the treatment of which direct pulp coating is performed, in the WHO classification should include only that form of initial pulpitis in which an accidental opening of the pulp cavity occurred during trauma to an intact tooth or during the treatment of dense and uninfected layers of mantle dentin in the treatment of, for example,medium caries . In this case, it is indeed the initial inflammation of the pulp (hyperemia), since the pulp was not infected and inflamed directly by microorganisms before opening.
It is this form of pulpitis that fully corresponds to the concept of "initial pulpitis", because in this case one does not have to guess whether it is caries or pulpitis and what is the main cause and onset of pulpitis. If it is possible to prevent the penetration of microorganisms into the tooth pulp in time through a defect up to 3 mm in size as a result of direct capping of the pulp with therapeutic pads, then it will be possible to preserve the pulp.
Moreover, an important factor influencing the outcome of treatment is the control of pulpary bleeding, the prolonged course of which indicates a more pronounced inflammation in the pulp, accompanied by a decrease in the reparative potential of the pulp. Such bleeding leads to microbial contamination of the dentin adjacent to the damaged pulp and makes it impossible to achieve adequate and high-quality tightness of the entire restoration, which will prevent subsequent infection with the microflora of the oral cavity.
At the same time, it is important to note that bleeding inside the root canal leads to a steady influx of stem cells, and bacteria and their toxins play a key role in direct stimulation of pulp cells and stem cells. In addition, a 1.5% solution of sodium hypochlorite (NaOCl) followed by the use of 17% EDTA solution, as well as corticosteroids, especially dexamethasone, have a positive effect on stem cells.
Thus, the success factors for direct pulp capping are: absence of signs of inflammation; hermetic restoration; control and stop of pulpary bleeding. If the defect is more than 3 mm, then the biological method of pulp treatment, as a rule, is not carried out and should be diagnosed as “traumatic pulpitis”, in the treatment of which the amputation or extirpation method of pulpitis treatment is carried .Clearly, the size of the outcrop area is essential (Mejare & Cvek 1993, Dammaschke et al. 2010). One study showed that when the opening was large (> 3 mm), direct coating was unsuccessful (Chailertvanitkul et al. 2014).
At the same time, if there was a perforation of the pulp during the evacuation of completely softened infected circumpulpal dentin, then direct coating of the pulp is not recommended, since in this case we do not have an initial inflammation of the pulp in the form of hyperemia, but an already developed inflammation of the pulp complicated by injury . In this case, if a pulp that has undergone purulent decomposition with the appearance of pus droplets and other destructive processes is objectively detected through the perforation hole, then the diagnosis, despite the absence of pain, definitely shifts towards pulpitis and it is preferable to carry out not amputation, but extirpation treatment of pulpitis – the only reliable method of treating this pathology.
If destructive changes in the pulp are not objectively observed, then it is possible to carry out a "pulpotomy" technique.Moreover, it is desirable to carry out the technique of "full pulpotomy", since it is more reliable than the technique "partial pulpotomy", in which it is difficult to determine the volume of the removed crown pulp.
Indirect pulp capping is carried out only with an unopened pulp cavity, when the demineralized infected circumpulpal dentin is maximally removed and the tooth pulp is separated from the bottom of the prepared cavity by a thin layer of circumpulpal dentin (dentine bridge). In this case, it is illogical to diagnose initial pulpitis or pulp hyperemia, since once sclerosed and reparative dentin has not been formed, then microorganisms and toxic products of their vital activity have definitely already penetrated into the tooth pulp from infected circumpulpal dentin, as a result of which the pulp is susceptible not to initial, but already chronic inflammation.That is why therapeutic pads are used to eliminate the inflammatory process in the pulp.
Thus, indirect pulp capping is performed when the pulp is already inflamed and not when there is hyperemia (see below).
In case of successful exposure of the material of therapeutic pads to the inflamed pulp, the deposition of sclerosed and reparative dentin occurs, which prevents further infection of the pulp.It was found that after the preparation of the carious cavity, the deposition rate of these protective layers averaged 1.4 microns per day. Moreover, the highest deposition rate is recorded in the first month after the indirect coating of the pulp, and after 48 days it steadily decreases.
Based on this, a rather paradoxical situation arises when, in the WHO classification of pulpitis, pathology really with initial inflammation of the pulp (hyperemia), for which direct capping is used, and pathology with clearly developed chronic inflammation of the pulp, for which indirect capping is used, are attributed to the same nosology "initial pulpitis". Is such a tactic acceptable and does not violate the generally accepted principles construction of classification in medicine?
In this case, nosology, in which direct capping is carried out, is certainly correctly attributed to "initial pulpitis", but nosology, which is characterized by already developed inflammation of the pulp and for the treatment of which indirect capping is carried out, in this case it would be more logical to refer to chronic forms of pulpitis in the WHO classification, rather than initial pulpitis.However, then, paradoxically, a logical question arises – to which nosology of chronic pulpitis should this rather unpredictable pathology be attributed from the point of view of treatment, in which the pulp is not removed, as a result of which it is difficult to make an accurate diagnosis, since it is impossible to assess the visual state of the extirpated pulp – the main object of diagnosis ?
Unambiguously unpredictable, since it is impossible to accurately predict whether, as a result of indirect capping of the pulp, it will be possible to finally prevent the transformation of caries into developed pulpitis, keeping the pulp viable.That is why in this case it is more logical to make a long-term preliminary diagnosis (this concept is found for the first time in the scientific literature, and the word "long-term" indicates the duration of determining the result of treatment), rather than a final diagnosis.
Since the main therapeutic actions are aimed at treating caries that caused inflammation of the pulp, it is more logical to first make a preliminary diagnosis of "progressive dentine caries".If, after indirect capping of the pulp and applying a temporary seal for some time (several weeks), the patient's complaints completely disappear and there is no exacerbation of the process, then this diagnosis becomes final and a permanent seal is placed.If during this time it is not possible to prevent the final transformation of caries into pulpitis and an exacerbation of the process occurs, then this nosology, depending on the developed clinical picture, should be attributed to one of the forms of developed pulpitis, and not to caries and especially not to initial pulpitis.
It is also illogical to make a final diagnosis of “reversible pulpitis” in such a situation, erroneously assuming the mythical transformation of the alleged pulpitis into caries, if such a transformation does not occur, then diagnose “irreversible pulpitis”.Based on all of the above, it is certainly advisable to consider progressive dentin caries, in which it was possible to prevent the complete transformation of caries into pulpitis, and not vice versa, as a transitional form between caries and pulpitis.
The belonging of this nosology to caries is confirmed by the unopened cavity of the tooth, the absence of spontaneous pain (clinical component). The morphologic picture may indicate a variety of forms of inflammation in different parts of the pulp (morphologic component).Since morphological studies of such pathology are not carried out in the clinic, and the treatment of this nosology (indirect pulp coating) is carried out with an unopened tooth cavity while preserving the pulp in the cured carious tooth, the main emphasis in the diagnosis of this form is placed on the clinical component.
Thus, in the diagnosis of progressive caries, one of the most important factors is to determine the reversibility or irreversibility of inflammation in the pulp tissues, and not the fact of the developed inflammation itself, the development of which can be stopped due to the reparative properties of the pulp.Therefore, this circumstance is the key moment both in diagnosis and in the choice of treatment method.
Thus, due to the unique protective and regenerative potential of the pulp, as a result of which the developed inflammation in the pulp tissues does not always lead to irreversible processes, its preservation is possible, which is confirmed in a number of studies.This is also evidenced by cured teeth with an open inflamed pulp, which have even undergone an amputation method of pulpitis treatment.Consequently, the main goals of biological caries treatment are to combat bacterial contamination, stop the development of caries, stimulate the formation of tertiary dentin and promote pulp restoration, as well as restore the tooth with a solid restoration for the long-term functioning of an asymptomatic functioning tooth with a healthy pulp (Duncan et al. 2019).
In this regard, the research of Levin L.G. deserves attention, who found that pulpitis usually becomes irreversible when the pulp has pronounced inflammation with signs of necrosis, which already makes it impossible to use a biological treatment method.
I will say more, the transformation of caries into pulpitis is sometimes prevented by nature itself even before the treatment of progressive caries as a result of the formation of sclerosed and replacement dentin by the body's defenses, which prevent the penetration of microbes and their waste products from the disintegrated infused periculpar dentin into the tooth pulp.After all, that is why it is illogical to diagnose such a form of caries, in which nature itself prevented the transformation of caries into pulpitis, as "initial pulpitis" according to the WHO classification and generally use therapeutic pads in this case.
MATERIALS AND METHODS
Let's take a closer look at the objective data and clinical manifestations of the nosology "progressive dentine caries", which in the classification of caries proposed by me, together with ordinary dentine caries and arrested dentine caries, is highlighted in the section "dentine caries"(https://dzen.ru/a/ZF8tnw6T3XDbSPzp).In my opinion, it is these forms of dentin caries that are the main forms of manifestation of the carious process in dentin, which are easily and reliably diagnosed.
The isolation of deep and extremely deep caries, I believe, definitely complicates diagnosis, since it is sometimes difficult to assess the different depth of the lesion by the carious process in linear and volumetric dimensions, which is due to variations in the thickness of hard tissues of different groups of teeth in different areas of the crown.At the same time, an X-ray assessment of the depth of the lesion does not allow to establish the exact depth of the lesion and the presence of protective layers of replacement dentin.In addition, the very linear interpretation of such a multifaceted and different pathology in its manifestations as caries does not really reflect the essence of the pathological and protective-adaptive processes taking place at the same time.
I am sure many clinicians agree with me that the choice of treatment for carious lesions depends not so much on the depth of the lesion, but on the quality of the tooth tissues remaining after the preparation of the carious cavity, especially since the classic carious process consists of five zones, not one. Because of this, during the formation of protective and adaptive layers of the carious process (sclerosed and replacement dentin), medium and deep caries are treated in the same way, since there is no need to use therapeutic pads.There is no doubt that it is easier to determine the presence or absence of protective layers of sclerosed and replacement dentin in the prepared cavity than the depth of the lesion, especially on the incisors of the lower jaw.
In progressive dentine caries, softened dentin from gray-yellow to black is found in the carious cavity, affecting the entire thickness of the parapulpal dentin.When probing, soreness is noted along the walls and bottom of the carious cavity, especially at the points closest to the pulp of the tooth.Patients complain of a cosmetic defect, food jamming, sharp pain resulting from the action of thermal, mechanical, chemical stimuli, disappearing immediately after their elimination (Fig.1).Radiologically, there are no special changes in the tissues surrounding the root of the tooth.These data make it possible to make only a preliminary diagnosis, and the final diagnosis is made only after the preparation of the carious cavity.

Fig.1. Progressive dentine caries.
As a result of removal of decayed tissues, we get a preprepared cavity within the circumpulpal dentin.Preparing and probing this cavity is sharply painful.The walls of this cavity are dense, while the bottom of the preprepared cavity (dentin bridge) is quite thin and elastic, and sometimes with signs of pigmentation and partial demineralization.In some cases, the pulp is slightly translucent through the thinning bottom of the cavity.
Probing the bottom of the cavity and removing demineralized softened dentin must be carried out very carefully, since in the places of projection of the pulp horns, the arch of the tooth cavity is very thin, therefore it is easy to pierce it with a probe, opening the tooth pulp, which is accompanied by sharp pain and the appearance of blood drops in the carious cavity.As a result, such pathology can no longer be considered caries and should be diagnosed in the section “pulpitis” . This clinical picture is associated with the lack of formation in the tooth of protective and adaptive layers of the carious process (sclerosed and reparative dentin).
Moreover, it should be noted that during the processing of the carious cavity, very soft dentin is easily removed, which can be removed with minimal resistance using hand tools, while slightly soft dentin is more resistant to removal.Hard and dense dentin is not amenable to scraping and therefore should not be removed.
It is also important to note that according to T. Fusayama, carious parapulpal dentin consists of two layers: external and internal.The outer layer is unable to remineralize due to direct bacterial infection and destruction of the collagen matrix.The inner layer, which is affected only by bacterial waste products with the integrity of the collagen matrix, is able to remineralize.Moreover, various cavities with a light-colored loose bottom are the most infected. Therefore, if the infected dentin is removed, the remaining demineralized dentin can be remineralized, and odontoblasts will form a replacement dentin, which will avoid pulp exposure.
However, based on many years of practical activity, I consider the Кореl tactic to be more acceptable, which allocates not two, but three layers of carious periculpar dentin :
1.Completely softened necrotic dentin, abundantly infected with bacteria.
2. Dense, slightly softened, demineralized dentin,
containing fewer bacteria.
3. Dense, not softened, often pigmented dentin,тpainful during processing, in which the content of bacteria is minimal, up to their possible absence.
Based on this, by completely removing demineralized parapulpal dentin with progressive caries, we obtain a prepared cavity with dense walls and a thin layer of periculpar dentin at the bottom.In this case, the arch of the pulp cavity (dentine bridge), in which the demineralized dentin is completely removed, usually represents a thin, dense septum, sometimes with signs of pigmentation (the third layer according to Korel).It is in this condition of the parapulpal dentine that it is desirable to carry out indirect coating of the pulp, completely removing demineralized dentin, avoiding opening the pulp.
However, unfortunately, this cannot be achieved in all cases, and therefore in some cases, in order to prevent the opening of the pulp, especially in the area of the horns of the pulp cavity, many clinicians leave a thin layer of partially demineralized dentin in this area..In this case, in their opinion, such softened dentin left does not particularly affect the condition of the pulp already infected with the microbes themselves, especially since in this situation, the protective and immune capabilities of the human body play an important role for successful treatment.In addition, in such a situation, in their opinion, the components of the therapeutic gasket act not only on the pulp tissue, but also on a thin layer of demineralized dentin, which sometimes, due to higher permeability, compared with dense layers of dentin, on the contrary, contributes to the unhindered penetration of the components of the therapeutic gasket into the pulp.
At the same time,they adhere to the statement of Shovelton, who in 1968 unequivocally stated that even if all softened demineralized dentin is completely removed, some of the microorganisms still remain in the dense layer of the dentine bridge.In addition, the formation of a protective layer of replacement dentin under a thin layer of softened demineralized dentin has long been convincingly proven.In animal models using healthy dentin, pulp tissue has been shown to have an innate ability to regenerate itself if the bacterial film is removed and the tooth is properly restored (Mjor & Tronstad 1974, Warfvinge & Bergenholtz 1986).Based on this, the modern division of carious dentin into affected and infected is, in principle, quite conditional.
I will say more, some modern studies on the treatment of deep carious lesions suggest that complete removal of soft dentin in order to leave a thin barrier of residual dentin may be unnecessary and even sometimes undesirable (Innes et al. 2016). The latter can be explained by a mechanical traumatic pulp injury that caused a "stress condition of the pulp". That is why the European Endodontic Society, in order to carry out an invasive treatment method for the treatment of such forms of caries, due to the fear of pulp opening, proposed selective (selective) one-stage and phased excavation of demineralized dentin, preventing pulp opening (ESE, 2019). Soft dentin remains locally only in the projection of the pulp horns, while carious dentin is removed from the periphery and central part of the cavity to a solid unchanged state.
The application of biomaterial to dentin with one-stage selective removal of carious tissues occurs after electoral necrectomy of soft dentin followed by permanent restoration.Step-by-step selective removal of carious tissues occurs in 2 visits in the interval of 6 months.The first step involves selective caries removal to slightly softened demineralized dentin (second layer according to Кореl) and application of biomaterial, and on the second visit, continuation of the necrectomy to hard modified dentin and final restoration.At the same time, ESE quite justifiably explains to patients the possibility of refusing such treatment due to a certain risk associated with the selective removal of demineralized dentin.
The opposite point of view is held by the American Association of Endodontists (AAE), as well as well-known clinician Professor Domenico Ricucci, German scientists E. Hellwig, J.Klimek, T. Attin, etc.. All of them unequivocally advise using indirect pulp coating (cuafage) only after non-selective removal of softened dentin (Fig.2) from the periphery and central part of the cavity to unchanged solid dentin (the third layer according to the Кореl).
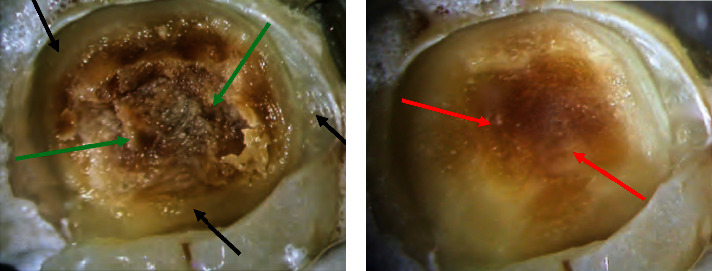
Fig.2. Non-selective removal of carious dentin (Warreth,2024):
1 – softened demineralized dentin (green arrows);
2 – its removal along the periphery (black arrows);
3 – its removal above the pulp cavity (red arrows).
Unfortunately, proponents of this technique do not even realize that what is the point in this case to carry out indirect pulp capping of the pulp at all, using therapeutic pads, if, thanks to the body's protective forces,sclerosed and reparative dentin has already been developed, as a result of which the circumpulpal dentin is dense, and sometimes even mineralized?After all, this is why experienced doctors in this situation never use therapeutic pads., and in the case of a thin dense dentine bridge, only protective linings are used to prevent the harmful effects of polymerization shrinkage during restoration with composites.
If the dentine bridge is quite dense and mineralized, then in this case there is no need to use even protective linings and it is enough to cover the circumpulpal dentine with an adhesive system, and then fill the cavity with a composite. Thus, is indirect pulp capping out only when using selective removal of carious dentin, therefore, supporters of the non-selective technique are deeply mistaken, persistently agitating to use indirect pulp capping with a selective technique.
In this regard, the statement of Sir John Tomes deserves attention, who stated back in 1859 that "it is better to leave a layer of pigmented and partially demineralized dentin to protect the pulp than to run the risk of sacrificing a tooth". Although it is difficult to strictly agree with this argument, since the risk of complications in the treatment of such lesions due to errors and difficulty in diagnosis is much higher than the probability of mineralization of demineralized softened dentin left due to fear of opening the pulp cavity!
The main danger lies in the fact that quite pathological destructive processes in the periapical region can occur against the background of a painless chronic course of such lesions.That is why such lesions must be monitored every year, especially by X-ray examinations.
During these preventive examinations, there should be no pain, symptoms of apical periodontitis (https://dzen.ru/a/ZF8b-kEW72xkS_ZA), signs of external and internal resorption, etc..If at least one of these symptoms is detected, then it is necessary to extirpate the pulp and seal the roots of the teeth qualitatively.
Based on many years of practical activity, I would like to note that in the treatment of such lesions and the choice of treatment, attention should be paid to the patient's age, his state of health, the presence of chronic odontogenic intoxication and pronounced periodontopathy, a decrease in the threshold of electrical excitability of the pulp below 40 mica of the tooth, the possibility of covering such teeth with orthopedic structures, the patient's solvency, etc.. It is these factors that sometimes dictate the choice of treatment tactics and the possibility of using selective and non-selective removal of demineralized dentin.
For example, if the patient's condition worsened at the time of treatment and there is a possibility of opening the pulp with complete removal of softened dentin, as a result of which it will be necessary to carry out a more traumatic extirpation treatment method that will be difficult for the patient to tolerate, then in this case, in order to avoid pain after opening the pulp, it is more advisable to leave the softened dentin for a biological treatment method.In addition, if the patient does not have the opportunity to pay for a more expensive pulp extirpation technique, then even then it is not worth risking removing the softened dentin. If a tooth with progressive dentine caries should be covered with orthopedic structures after treatment, then biological treatment methods should not be used to avoid complications.
I will say more, due to the refusal of some patients to completely remove the pulp, I sometimes had to carry out coating of the pulp after opening the pulp when removing softened demineralized circumpulpal dentin.However, paradoxically, the results of treatment of some patients turned out to be positive for many years.
By the way, the idea of leaving partially demineralized dentin above the vault of the pulp cavity belongs to the "father of modern dentistry" Pierre Fauchard (1678-1761).However, his justification for preserving carious dentin was based on his fear of exposing the “nerves” in the tooth, which, in his opinion, would lead to tooth destruction.In general, it is important to note that even an experienced clinician can only predict with a certain degree of probability the possibility of opening the pulp during the excavation of softened circumpulpal dentin.
It is especially difficult to do this when a dense layer of circumpulpal dentin has not been preserved at all.It is the presence or absence of this layer that determines the choice of a selective or non-selective method for removing softened dentin.Unfortunately, the presence of this layer is sometimes quite difficult to determine, which can lead to the opening of the pulp.All this, of course, makes it difficult to choose a treatment method. That is why selective removal of softened dentin is more justified in this case.In this regard, the words of Green Vardiman Black are instructive, who in 1908 said: "The question often arises whether the pulp will be exposed after the removal of all carious dentin".
Based on the above, it cannot be unequivocally stated that indirect capping pulp should be carried out only with non-selective removal of softened dentin, since sometimes, due to the prevailing circumstances, it is more advisable to leave a layer of slightly softened dentin(the selective method).
By the way, the first material for the therapeutic coating of the bottom of the carious cavity was gold. This technique was first described in 1756 by the personal dentist of the Prussian king Philip Pfaff. At the same time, one cannot fully hope for a favorable outcome of the biological treatment method, since many clinicians point out that the main component of therapeutic pads – calcium hydroxide with excessive coating can cause pulp necrosis. In addition, it does not have strong adhesion to dentin, decomposes over time, and has low compressive strength.
The most significant drawback, which, unfortunately, is not paid attention to by leading scientists and which is the cause of many treatment failures, is its inactivation as a result of interaction with chemical components of protective pads that have not yet hardened (see below ).
These properties of calcium hydroxide lead to micro-leakage and failures in the treatment of vital teeth. That is why, with the advent of bioactive cements based on calcium silicate (MTA) as a material with antimicrobial and remineralizing effects, in which calcium hydroxide is released after the hardening of the gasket from (MTA), the success of the biological treatment of progressive dentine caries has significantly increased. Biologically active Biodentine silicate also showed positive results.
At the same time, it should not be forgotten that calcium hydroxide, although less effective against some intracanal bacterial species than pastes with antibiotics, its use is associated with greater survival and proliferation of stem cells. It activates the cells of the pulp mesenchymal, as a result of which they differentiate into odontoblast-like cells, which prevents the destruction of the epithelial cells of the Gertwig vagina, however, some studies indicate the destruction of the epithelial cells of the Malasse islets (Terekhova T. N., 2021).
At the same time, conventional calcium hydroxide in the form of a paste should not be used, since when interacting with the chemical components of the hardening protective gasket, the therapeutic properties of the therapeutic gasket are inactivated. In this case, when directly coating the pulp, it is advisable to use calcium hydroxide powder, which is applied directly to the opened pulp, and a protective gasket made of glass ionomer cement is placed on the surface of the dentine bridge, which is not coated with calcium hydroxide.
When there were no pads of bioactive cements based on calcium silicate (MTA), using calcium hydroxide in the form of a paste to prevent the negative effects of the components of the protective gasket on it, I used sterile cellophane films of appropriate sizes to isolate the therapeutic gasket. Moreover, using this technique, there was no need to use a protective gasket and on the first visit, on top of a protective film cut exactly according to the configuration of the dentine bridge, the prepared cavity was filled with a temporary seal or glass ionomer cement (the latter is used especially if the configuration of the cavity is insufficient for long-term fixation of the temporary seal).
During the second visit, the temporary insulating material was easily removed along with the protective film, and in the case of dentin mineralization, the final restoration was carried out with composites or amalgam (Khidirbegishvili method). If, after removing the protective film, there were no traces of dentin mineralization, then the softened dentin was removed and the procedure similar to the first visit was performed again. In general, studies have shown that indirect pulp coating has a better prognosis than direct.
I would also like to express my opinion on the issue of the time of the second visit patient during the two-stage biological method. Based on many years of practical activity, I consider it unreasonable to conduct a second visit after 6 months, since it is often during this period that the final formation of protective and adaptive layers takes place. Even if they have not formed, it makes no sense to open the seal for additional removal of the remaining demineralized dentin, since this will not affect the outcome of treatment in any way.
In this case, the positive outcome of treatment may be influenced by the immune reactions of the body, which, due to the mineralization of the remaining pulp and periapical tissues, prevent further penetration of infection. Based on this, it is quite enough to conduct a second visit within one or two weeks and, if there is no aggravation of the process, then complete the restoration of the tooth. That is why, in this case, it is often quite enough to use temporary seals instead of permanent sealing materials on the first visit. After the expiration of 6 months to a year, even in the absence of complications, it is necessary to conduct an X-ray examination to exclude the occurrence of destructive processes in the bone tissue.
In this regard, it is difficult to agree with the indirect coating method, which is proposed in his book "Endodontology. An integrated biological and clinical view" by Professor Domenico Ricucci, since on the first visit he applies both a therapeutic and protective pad and temporarily seals fills the cavity with a composite or amalgam. And paradoxically, on the second visit, he removes such durable sealing materials as composite and amalgam, as well as a protective gasket, the removal of which, due to its proximity to the pulp cavity, is associated with its opening. In addition, Professor Ricucci, offering doctors a similar treatment method, unfortunately, does not take into account the inactivation of the chemical components of the therapeutic pad as a result of interaction with the components of the protective pad (see above).
I will say more, in his book Ricucci, oddly enough, tries to prove the presence of microorganisms in dense pigmented dentine. To prove this, in his book he describes a rather strange experiment with a carious tooth (Fig.3-2), which later for some reason had to be removed allegedly due to orthopedic indications due to dentoalveolar advancement (unfortunately,Ricucci, apparently due to a conflict of interest, did not allow me to publish this drawing). To do this, he prepared a shallow carious lesion in the fissure on the second molar of the upper jaw using a rather traumatic Black method, specifically leaving a dense pigmented layer of dentin at the bottom of the cavity. After tooth extraction, he prepared preparations for histological examination.
Having discovered the presence of microorganisms in dense pigmented dentin during histological examination, Ricucci was probably proud of his alleged discovery. However, paradoxically, the eminent scientist apparently forgot that the presence of microorganisms has long been proven not only in pigmented dense dentine, but even in solid non-pigmented dentine. At the same time, it has long been proven that this pigmented dentin, with timely and adequate treatment, does not pose a danger under restoration, as a result of which doctors all over the world never remove dense pigmented dentin in the treatment of such lesions.
Despite this, Ricucci is still skeptical about such dentin, loudly and inadequately stating in his book that when pigmented tissues are preserved, infected carious dentin remains under restoration, which increases the risk of recurrence and pulp damage ( p. 69). At the same time, Professor Ricucci writes in his book that even complete excision of carious tissues does not guarantee the removal of all microorganisms that can persist in solid dentine ( page 71). Thus out, that in this case, in the treatment of such lesions, the main thing is timely and adequate treatment, and not the presence of microorganisms in the prepared dentine.
In this case, conducting such a strange and, in fact, traumatic experiment, Professor Rikuchi would have been better, logically, to carry out indirect pulp capping followed by restoration for the time being, and then after tooth extraction. , he could conduct his favorite histological studies to once again verify the non-pathogenicity of microorganisms of dense pigmented dentin, of course, in the case of timely and adequate biological treatment.
At the same time, unfortunately, Mr. Ricucci, like many of his colleagues, does not realize what is the point in carrying out indirect coating of the pulp after carrying out a non — selective method of removing carious dentin, if the dentine bridge in this case is already dense, and sometimes even mineralized due to the protective forces of the body.
In any case, I just feel sorry for this extracted tooth, which, even at the expense of dentoalveolar expansion, of course, could have been easily preserved (at least preserved healthy filled roots), and not removed for the sake of this useless experiment.
In addition, it is difficult to agree with a colleague who considers such a lesion to be an initial carious lesion, especially after its preparation. At the same time, in my opinion, it is impermissible to distinguish superficial, medium and deep caries in this book, since it is usually customary to distinguish: the spot stage, superficial caries, medium caries and deep caries. This is due to the fact that the spot stage is significantly different from the listed forms of caries and only the white spot (the initial clinical manifestation of caries) and the pigmented spot belong to it. It is these enamel lesions that are considered the initial carious lesions, and not superficial caries, which cannot be differentiated from a pigmented spot.
If we consider that the average thickness of the enamel in different parts of the tooth is from 0.6 – 3 mm, and at the level of the neck of the tooth ends altogether, then we just have to "envy" clinicians who manage not only to diagnose superficial caries, but also to seal it without fixing the seal in the mantle dentine (dentine caries). That is why during many years of practice I have never been able to diagnose superficial caries. Based on this, the allocation of superficial enamel caries in the classification of caries is simply impractical.
It is also important to note that in this book by Professor Ricucci it is also difficult to agree with his statement that, since the treatment of granulomas and cysts is the same and histological examination is not always used in their diagnosis, it makes no sense to differentiate these lesions. Apparently, the famous scientist forgot that after resection or tooth extraction, histological examination of cysts and granulomas is often performed to exclude oncological pathology. As for the differentiation of these lesions with successful endodontic treatment, my tactics of their diagnosis in my article deserves attention ( https://dzen.ru/a/ZF8b-kEW72xkS_ZA ).
In addition, oddly enough, Mr. Ricucci for some reason considers the obturation of the lateral canals unnecessary due to the alleged presence of infection in the main central canal of the tooth. At the same time, he does not always consider tool failure, poor-quality canal filling, perforation of the canal, etc. to be the cause of complications, since the main cause of complications, in his opinion, is the persistence of infection in the root canal system. It is because of these significant omissions of Professor Ricucci that I am preparing a separate article in which they will be covered in more detail so that practicing doctors avoid serious complications and correctly assess the clinical situation.
It should also be noted that during the final sealing of such lesions, if after the expiration of time under a temporary seal with a therapeutic pad, the dentine bridge of the vault of the pulp chamber has not mineralized, then it should not be covered directly with light-curing adhesive systems and composites. In this case, the danger is the negative effect of increased polymerization shrinkage of these materials on the tooth pulp. Therefore, in this case, these materials should be used after fixing the protective pads of chemical curing(glass ionomer cements), which have a slight polymerization shrinkage. Based on this, a step-by-step method of indirect coating of pulp and excavation of demineralized dentin is more justified.
I will say more, based on the above, over many years of practical activity, I have successfully used silver amalgam as both therapeutic and protective pads, which I applied with a thin layer to the dentine bridge and after its slight hardening I carried out the restoration of the prepared cavity with composite materials. The positive outcome of such treatment was due to the lowest polymerization shrinkage of amalgam among filling materials, tight edge fit, and antibacterial properties (Khidirbegishvili method).
However, the most positive property of this material is that it is perhaps the only restoration material that microorganisms, due to the presence of mercury in the amalgam, do not use as a nutrient substrate and therefore quickly inactivate. After all, that is why secondary caries practically does not occur on the amalgam. By the way, in Soviet times, when there were no reliable antiseptic pastes and root sealers for disinfection of periapical tissues, I filled the apex of the root with amalgam and only then filled the canal with a sealer(Khidirbegishvili method).
Unfortunately, the debate about selective or non-selective removal of demineralized dentin has not stopped yet, and in recent years, supporters of selective caries removal have been fiercely opposed by the AAE and especially by Professor Domenico Ricucci, who at his annual endodontic forums Endo Sapiens persistently agitates clinicians only for the use of non-selective removal of carious dentin!
At the same time, the International Consensus Cooperation on Caries (a group of 21 experts from 12 countries), which met in Belgium in 2015, came to a consensus that complete removal of carious tissue to hard dentin is excessive treatment, and advocated selective, phased removal of carious tissue. At the same time, the European Society of Endodontists has published a statement on a position that further strengthens the selective removal of carious dentin in teeth with reversible pulpitis.
In this statement, the rationale for selective caries removal is based on the results obtained in recent clinical studies.According to these studies, bacteria isolated from a food source by restoring sufficient integrity either die or remain dormant, thereby creating minimal risk to the pulp.
On this basis, a new clinical approach for selective caries removal has been proposed.The technique consists in removing only the surface layers of soft dentin and leaving the carious dentin hard and leathery on the surface of the pulp. Moreover, the soft dentin is removed with hand tools and with the help of low-speed burs until the underlying dentin becomes solid during probing.In this state, bacteria isolated from nutrients by sclerosed and substitutive dentin are trapped and actually in a "stressful environment"(Duncan et al. 2019).
RESULTS AND DISCUSSION
This is definitely the most unfavorable and unpredictable form of dentin caries both in terms of diagnosis and treatment, since it is impossible to accurately determine the type and degree of inflammation of the pulp and the possibility of its further functioning! In this respect, the statements about such carious lesions of scientists M. Bushan and V. Kulazhenko, who in the book “Dental caries, its treatment and prevention with the use of vacuum electrophoresis” (1975) unambiguously stated that this condition is actually a transitional form between caries and pulpitis and is diagnosed as deep caries with hyperemia.
Regarding the transitional form, of course, we can agree, but with such a pronounced pathological decay of parapulpal dentin, it is difficult to agree on the hyperemia of the pulp, which is the initial form of inflammation of the pulp, developed in the early stages of the carious process.
As is known, inflammation in the pulp occurs immediately as soon as the carious process affects the tooth enamel (Simon, 1972).At this stage of the development of the carious process, the vessels of the pulp expand and individual inflammatory cells (lymphocytes, plasma cells, etc.) can be detected, but not in such numbers as to classify them as inflammatory exudate (Fig.3).All these cells are involved in immune, regenerative, and trophic reactions. Moreover, microbial toxins, enzymes, and antigens enter the pulp earlier than the bacteria themselves (Trowbridge, 1972).
Figure 3. Initial pulp inflammation (pulp hyperemia) :
1 - reparative dentin; 2 - demineralized dentin; 3 - single inflammatory cells; 4 - dilated vessels; 5 - non-inflamed pulp.
Such inflammation is considered to be initial, significantly different from severe inflammation of the pulp (pulpitis), when bacteria directly penetrate into the pulp of the tooth.It was precisely this mechanism of protection against infection that Seltzer considered the initial inflammation, which he called "pulp hyperemia" and considered a transitional stage from the initial inflammatory process to advanced pulp inflammation.
In fact, pulp hyperemia is a consequence of the initial impact on the pulp of various stimuli of the carious process and to one degree or another occurs in many forms of caries, especially in those where there is no need to use an indirect coating, which is carried out only with advanced inflammation of the pulp.In addition, if it is possible to eliminate the carious process in time before the deep layers of the parapulpal dentin are affected, the hyperemia immediately passes.
In addition, pulp hyperemia is found not only in caries, but also in the preparation of the carious cavity, pathological erasability, various periodontal diseases, etc. Therefore, hyperemia is not a nosology, but only a symptom found in various diseases, as a result of which it makes no sense to single it out in the WHO classification of pulpitis.
At the same time, the protective initial inflammation is based on the immune mechanism and the inflammatory-reparative process, which is both a response and a protective reaction of the dentin-pulp complex to the penetration of microbial waste products into the tooth pulp.The first and most common reaction of the pulp to caries is dentin sclerosis, as a result of which the dentine tubules are partially or completely filled with deposits of peritubular dentin, which affects the permeability of dentin.The next mechanism for protecting the pulp from infection is its production of replacement dentin, which isolates the pulp from infected dentin.It is these protective and adaptive layers that limit the diffusion of inflammatory substances and microorganisms into the tooth pulp.
At the same time, during the deposition of replacement dentin on the walls of the pulp cavity, the pulp volume decreases, the collagen part increases and the cellular composition decreases, resulting in a decrease in its functions.This condition is called "pulp atrophy" and it is in this condition that the pulp often functions after successful treatment with a biological method of pulp treatment, when sclerosed and reparative dentin has been developed under the influence of a therapeutic pad (Fig.4).
If these protective layers of dentin have not formed, as a result of which pulp atrophy has not occurred, then in this case it is impossible to prevent the progression of the carious process into developed pulpitis.
Fig.4.Scheme of reparative-inflammatory process in the dental pulp.
Thus, the inflamed pulp never returns to its original non-inflamed state, however, in a state of atrophy, it can still function in a cured carious tooth. At the same time, it is important to always remember that as a result of the biological treatment method, the pulp can completely mineralize (fibrous pulpitis) or completely necrotize (pulp necrosis),but even in this condition of the pulp, the tooth can function for a long time due to natural immune protective and adaptive processes in the periapical tissues.
Unfortunately, the initial inflammation does not always lead to the formation of protective and adaptive layers of replacement dentin and with the progression of the carious process(Fig.5) pulp hyperemia directly passes into various forms of developed inflammation of the pulp.Moreover, the closer the carious process to the pulp of the tooth, the more pronounced is the resulting inflammation.If chronic forms of pulp inflammation prevail, this is indirectly evidenced by the following factors: a long-term carious process with pathological destruction of periculpar dentin, absence of pain (chronic course), absence of protective and adaptive layers of the carious process (sclerosed and substitutive dentin). After all, that is why it is difficult to preserve such an inflamed pulp by a biological treatment method.
Fig.5. Stages of carious process progression.
Unfortunately, without morphological studies, which are not carried out in the clinic, it is impossible to accurately determine the condition of the pulp and even more so to determine the moment of transition of hyperemia into pronounced inflammation of the pulp.At the same time, progressive and suspended processes in the pulp can occur simultaneously, and various forms of pulp inflammation can be detected in different areas of the pulp.In addition, it is impossible to establish a correlation between clinical manifestations and morphological data of the pulp.Attempts to link the nature of pain with the condition of the pulp were unsuccessful, because, according to Simon, there is no correlation between the severity of pain and the degree of damage to the pulp.
After all, that is why clinicians V.S. Ivanov and L. I. Urbanovich quite reasonably argued that the biological method is discredited not because it is not possible to keep the pulp viable, but because it is impossible to accurately identify the degree and stage of inflammation of the pulp.
Unfortunately, the modern method of diagnosing the reversibility or irreversibility of an inflamed pulp using biological markers of inflammation has not yet fully justified itself. Nevertheless, further studies using more accurate control methods using an autofluorescence diagnostic device (AFS), which allows selectively removing infected dentin by visualizing areas of bacterial invasion, do not stop. The method has shown some effectiveness in differentiating affected and infected dentin by the nature of fluorescence of parapulpal dentin (healthy tissues — green glow, dense dentin — orange glow, soft infected dentin — red).
Based on this, there is still no reliable standard non-invasive method for accurately assessing the condition of the pulp, as a result of which the main criteria for using the biological method in the first place are: the absence of spontaneous pain, the absence of pain during percussion, the integrity of the bottom of the pulp chamber, an open tooth cavity up to 3 mm, the absence of adjacent pathologies, the absence of destructive changes in bone tissue, etc..
The main criteria for refusing to carry out the biological method of carrying out are: spontaneous pain both during the day and at night , pain during percussion, an open tooth cavity of more than 3 mm, the presence of adjacent pathologies, destructive changes in bone tissue, the possibility of using orthopedic structures, etc..
At the same time, during diagnosis, the emphasis should not be placed on the alleged reverse transformation of pulpitis into caries (reversible pulpitis), but, on the contrary, on the possibility of preventing the progressive transformation of caries into developed pulpitis.In addition, it is difficult to agree with the American Association of Endodontists (AAE), which uses the terms "reversible pulpitis" and "irreversible pulpitis" for diagnosis, since it seems that with reversible pulpitis, pulpitis transforms into caries, and with irreversible pulpitis remains pulpitis.
At the same time, it is unacceptable to diagnose such a common and pathological disease as "pulpitis" by such a simplified method, without highlighting the numerous forms of this pathology.That is why we should
agree with the current CEO of ESE, Professor Duncan H. F., who unequivocally stated the need to review these AAE nosologies(Duncan et al. 2019).
In this regard, it should also be noted that the only form of pulpitis, the diagnosis of which can easily determine its "irreversibility", is hypertrophic pulpitis.This is clearly evidenced by the objective picture of the pulp itself.Unfortunately, dentistry is the only field of medicine in which the diagnosis of the removed organ (pulp) does not use objective data of the main object of diagnosis.That is why, in order to correct such an unacceptable situation, I propose a classification of pulpitis, in which the diagnosis is made on the basis of objective data from the extirpated pulp (https://dzen.ru/a/ZF5UQ0ej8SbfgCyY ). Only this method of classification construction does not violate the generally accepted diagnostic tactics for surgical interventions.
Moreover, in this classification, holistic (unitary) forms of pulpitis are distinguished, in which biological methods of pulp preservation can be carried out, and destructive forms, in which only extirpacil methods of pulpitis treatment are introduced.Such tactics make it easier to choose a treatment method.
Thus, it is advisable to consider progressive dentine caries as a transitional form between caries and pulpitis.This approach is also justified by the fact that it becomes possible to justify the legal responsibility of a doctor in the treatment of such a neglected form of caries, since by fixing such a diagnosis and warning the patient in advance of possible complications, the doctor, in case of an exacerbation of the process, relieves himself of legal responsibility if adequate treatment has been carried out.In this case, with the consent of the patient, the doctor, taking into account the body's defenses, I did everything possible to prevent the complete transformation of caries into pulpitis.
At the same time, the term "transitional form" in this case is justified, since whether caries has transformed into developed pulpitis or it will be possible to prevent such a transformation with modern treatment methods is largely determined by the characteristics of the body's protective system.It is precisely this function of our body that can sometimes unambiguously explain the positive outcome of treatment of this neglected form of caries.
CONCLUSION
Based on all of the above, progressive forms of dentin caries cannot be placed in the WHO classification of pulpitis.In this regard, how prophetic was the tactics of Russian scientists, who, unlike the creators of the WHO classification, half a century ago quite reasonably proposed to take into account the transitional form between caries and pulpitis, referring this nosology to caries, and not to the initial pulpitis, as it is still unambiguously mistakenly proposed in the WHO classification of pulpitis.
If the significant shortcomings of the WHO classification are not corrected, then dentistry will turn out to be, perhaps, the only medical discipline in which practically the same nosology in different classifications will be attributed simultaneously to two completely different diseases (caries and pulpitis)!
I will say more, all existing classifications of caries, pulp diseases and periodontitis must be modernized, otherwise clinicians around the world will again make unacceptable diagnostic errors. That is why, in order to modernize them, I propose to use the classifications of these diseases that I have proposed.
In conclusion, I invite clinicians and all interested parties to participate in a discussion of these classifications and the possibility of their use in clinical practice.
I will gratefully accept and take into account all the amendments and recommendations sent by you (otari@inbox.ru).
Conflict of interests. The author declare no conflict of interests
Otari Eduardovich Khidirbegishvili is a graduate of the SSMI in 1978, who has been engaged in practical, scientific and pedagogical activities in the city of Tbilisi for more than forty years. During this time, more than 100 articles have been published in leading dental journals, and in 2005 the Dental Association of Russia published a monograph "Modern Cariesology", which is accepted for teaching in Russia and in many countries. Due to developments in the field of theoretical dentistry, the photo is placed on the cover of the Russian magazine "Maestro of Dentistry" (№ 1(10)2003).
REFERENCES
1.Bader JD, Shugars DA, Bonito AJ. 2001. Systematic reviews of selected dental caries diagnostic and management methods. J Dent Edu. 65(10):960-968.
2.Baelum V, Hintze H, Wenzel A, Danielsen B, Nyvad B. 2012. Implications of caries diagnostic strategies for clinical management decisions. Community Dent Oral Epidemiol. 40(3):257-266.
3.Banerjee A, Kidd EA, Watson TF. 2000. In vitro evaluation of five alternative methods of carious dentine excavation. Caries Res. 34(2):144-150.
4.Bjørndal L, Demant S, Dabelsteen S. 2014. Depth and activity of carious lesions as indicators for the regenerative potential of dental pulp after intervention. J Endod. 40(4 Suppl):76S-81S
5.De Munck J, Van Meerbeek B, Yoshida Y, Inoue S, Vargas M, Suzuki K, Lambrechts P, Vanherle G. 2003. Four-year water degradation of total-etch adhesives bonded to dentin. J Dent Res. 82(2):136-140.
6.Fusayama T. 1997. The process and results of revolution in dental caries treatment. Int Dent J. 47(3):157-166. Fusayama T, Kurosaki N. 1972. Structure and removal of carious dentin. Int Dent J. 22(3):401-411
7.Kidd EA, Joyston-Bechal S, Beighton D. 1993. Microbiological validation of assessments of caries activity during cavity preparation. Caries Res. 27(5):402-408.
8.Ngo HC, Mount G, Mc Intyre J, Tuisuva J, Von Doussa RJ. 2006. Chemical exchange between glass-ionomer restorations and residual carious dentine in permanent molars: An in vivo study. J Dent. 34(8):608-613.
9.Paddick JS, Brailsford SR, Kidd EA, Beighton D. 2005. Phenotypic and genotypic selection of microbiota surviving under dental restorations. Appl Environ Microbiol. 71(5):2467-2472.
10.Orhan AI, Oz FT, Orhan K. 2010. Pulp exposure occurrence and outcomes after 1- or 2-visit indirect pulp therapy vs complete caries removal in primary and permanent molars. Pediatr Dent. 32(4):347-355.
11.Munson MA, Banerjee A, Watson TF, Wade WG. 2004. Molecular analysis of the microflora associated with dental caries. J Clin Microbiol. 42(7):3023-3029.
12.Manhart J, Chen HY, Hamm G, Hickel, R. 2004. Review of the clinical survival of direct and indirect restorations in posterior teeth of the permanent dentition. Oper Dent. 29(5):481-508.
13.Mejare IA, Axelsson S, Davidson T, Frisk F, Hakeberg M, Kvist T, Norlund A, Petersson A, Portenier I, Sandberg H et al. 2012. Diagnosis of the condition of the dental pulp: A systematic review. Int Endod J. 45(7):597-613.
14.Elderton RJ. 1993. Overtreatment with restorative dentistry: When to intervene? Int Dent J. 43(1):17-24.