
Старый и удлиненнный ваиант !
Khidirbegishvili O.E.
Dentist. Tbilisi, Georgia
Private dental clinic
Annotation The article presents the literature data on the modernization of the classification of caries.The disadvantages of the applied classifications, including the WHO classification, are described, new nosological forms are proposed and the principles of constructing a modern working classification of caries are formulated.
Keywords: enamel caries, medium caries, deep caries, progressive dentine caries, initial pulpitis, cement caries.
INTRODUCTION
Dental caries is considered one of the oldest and most common human diseases.The history of dentistry dates back to 5000 BC, when it was believed that the cause of caries was a "toothworm". The term "dental caries" first appeared in literature around 1634 and comes from the Latin word "caries", which means decay, destruction of the tooth.
At the same time, modern cariesology has reached a sufficient level of development to provide clinicians with adequate knowledge in the field of etiology, clinic and treatment of caries.However, strangely enough, there is still no clinical classification of caries that fully meets the requirements of clinicians.I will say more, considering some of the classifications used in different countries, it is amazing how different and contradictory they are, and sometimes it even seems that we live on different planets.
The clinical classification of caries based on the depth of the lesion (initial caries, superficial caries, medium caries, deep caries) does not properly reflect the variety of forms of carious process manifestation and does not provide sufficient information about the state of the tissues affected by caries. This classification was proposed in 1948 by I.G. Lukomsky and was intended for the use of cements and amalgams, not composites, which appeared on the market only in 1962. At the same time, when using it, it is sometimes difficult to assess the different depths of carious lesions by linear and volumetric dimensions, which is associated with variations in the thickness of hard tissues of different groups of teeth in different areas of the crown.
In addition, the very linear interpretation of a pathology as multifaceted and varied in its manifestations as caries does not really reflect the essence of the pathological and protective-adaptive processes occurring in this case.It is unlikely that I.G. Lukomsky would have proposed such a classification if at that time there had been adhesive systems and modern filling materials, the use of which depends not so much on the depth of the lesion, but on the quality of the tooth tissue remaining after the preparation of the carious cavity, especially since the classic The carious process consists of five zones, not one (Fig. 1).
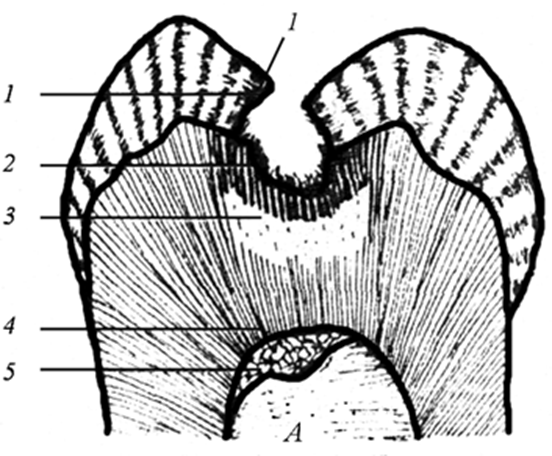
Fig.1.Zones of carious process in dentin ( A.V.Borisenko, 2000).
1. Decay zone.
2. Zone of demineralization.
3. Zone of transparent (sclerosized) dentin.
4. Zone of apparently unchanged (conditionally intact) dentin.
5. Zone of secondary (replacement) dentin.
After all, that is why, with the formation of protective and adaptive layers of the carious process (sclerosed and replacement dentin), medium and deep caries are treated in the same way, since there is no need to use therapeutic pads.It turns out that in this case, the depth of the lesion is absolutely irrelevant and therefore there is no need to separately classify such lesions according to the depth of the carious process.
That is why it is difficult to agree with the American Dental Association (ADA) and the European Endodontic Society (ESE), which pay special attention to the depth of the lesion, highlighting not only deep caries, but also very deep caries (extremely deep caries). I will say more, the ADA calls such a progressive form of carious lesion that spreads to the pulp chamber and even to the root canal system (in this case it is already a form of pulpitis or periodontitis) as endodontic caries or root canal caries. These well-known organizations, strangely enough, pay attention not to the presence or absence of protective and adaptive layers of the carious process, on which directly depends on the diagnosis and treatment tactics, and erroneously the immediate depth of the lesion.
In addition, using both topographic classification and other classifications of caries, many clinicians make the final diagnosis of a particular form of caries, oddly enough, based on the data of anamnesis, patient complaints and the objective state of the carious cavity. Paradoxically, but in textbooks in the section “Clinic and Diagnosis of Caries” described only objective pictures of carious cavities, and otpreprepare cavities, which are different for each form of caries, is not paid attention at all.
Such tactics in many cases leads to diagnostic errors, because the degree of depth of the carious process and the quality of the remaining tissues of the tooth can be established only after a quality preparation of the tooth. And only then you can make a final diagnosis and choose the appropriate method of caries treatment!
By refusing such tactics, the principle of diagnosis at surgical interventions, generally accepted in medicine, is violated, which states that on the basis of the patient's complaints and objective state of the carious cavity only a preliminary diagnosis is made, and the final diagnosis - only after surgical intervention! That is why my monograph “Modern Cariesology” describes in detail the possible variants of reprepared carious cavities.
This is probably why some clinicians, without dissecting the carious lesion, erroneously make, for example, the diagnosis of “superficial caries” and even sometimes manage to fill such insignificant in thickness cavities! If we take into account that the average thickness of enamel in different parts of the tooth from 0.6 - 3 mm, and at the level of the neck of the tooth and ends altogether, we must simply “envy” the art of doctoring clinicians who manage not only to diagnose superficial caries, but also to fill it without fixing the filling in the clad dentin (dentin caries). Nothing to say, these clinicians are worthy students of their “advanced” teachers, because I during many years of practice has not been able to diagnose superficial caries.
It is also important that the topographic classification takes into account the course of carious process only in enamel and dentin, as a result of which it does not pay attention to the carious process in cementum, the clinic and treatment of which has its own features. Therefore, in modern conditions it is necessary to classify caries, which would reflect not only the quality of tissues affected by carious process, but also take into account the features of the course of carious process in enamel, dentin and cementum.
As is known, such a course of carious process in various tissues of the tooth is considered in the WHO anatomical classification (ICD-10).The undoubted advantage of this classification is not only the consideration of the peculiarities of the clinical course and treatment of the carious process in cementum, but also the exclusion of the nosology “superficial caries” from the clinical manifestations of the carious process in enamel!
However, despite certain advantages, unfortunately, the WHO classification is also not without drawbacks. First of all, I would like to express my disagreement with the use of the term “initial caries” to denote the initial clinical manifestations of enamel caries (white spot). This approach is due to the fact that initial caries should be considered as the result of numerous changes within the enamel, which are not registered in the clinic and which occur during the maturation of the dental plaque.That is why it is logical to call the white spot the initial clinical manifestation of caries, not the initial caries!
A significant disadvantage in the WHO classification is also the interpretation of enamel caries, in which only the white spot stage is distinguished, and the pigmented spot, which is also characterized by the integrity of the enamel-dentine border, is singled out separately as arrested enamel caries.
I would also like to note that the WHO clinical classification does not take into account the topographic and qualitative characteristics of the pathological and protective-adaptive zones of the carious process. That is why it is impossible to agree with the identification of only one form of dentin caries in the WHO classification!Is indirect pulp plating, sandwich technique, layered restoration technique and Bertolucci technique performed with the same form of dentin caries? Based on this, it is advisable to supplement the WHO classification with topographic and qualitative characteristics of dental tissues involved in the carious process.
It is also difficult to agree with the lack of separate isolation of various forms of arrested caries in dentin and cement, the treatments of which are different and have their own characteristics.As for the concept of the suspended course of caries in various tooth tissues, it has changed repeatedly over the years.For example, Lukomsky I.G. (1948) only pigmented spots without damage to the enamel-dentine junction to be arrested caries.
At the same time, prominent Soviet scientists Rybakov A.I. and Kodola N.A. unequivocally proved that the development of the carious process at any stage of development can be suspended due to increased hypermineralization of tooth tissues.
It is important to note that this concept was adhered to by supporters of the isolation of acute and chronic caries, because they consider arrested caries to be a kind of chronic course of the carious process in various tissues of the tooth.Thus, in the clinical classification of caries, it is necessary to separately identify arrested caries not only of enamel, but of dentin and cement, for the treatment of which various treatment methods are used.
Allocation in the WHO classification of only one form of arrested caries (pigmented spot) is clearly insufficient. Is it in such a complex and multifaceted in its manifestations of pathological process as caries Mother Nature has not provided a mechanism to protect not only the spread of carious process from enamel to dentin (pigmented spot), but also from the crown and root dentin to the pulp.
Moreover, many clinicians, making the diagnosis of “arrested caries” according to the WHO classification, put the emphasis not on the protective hypermineralization of the pigmented spot, delaying the progression of caries, for example, in the fissures, but on the long-term not formed visible carious defect. It is on this basis, some clinicians in their classifications emphasize carious demineralization and carious defect (classification of MMSI).
I think it is difficult to agree with this tactic, because the absence of a visible carious defect in carious enamel demineralization does not always indicate stabilization of the process.Often, when dissecting such lesions, various lesions of different dentin layers (dentin caries) are often found, which are characterized by various filling techniques.
I will say more, when pigmented spots are localized in fissures, the carious process progresses relatively quickly into dentine, since their bottom almost reaches the enamel-dentine border, as a result of which it is difficult to trace the transition of the process from enamel to dentine (Fig.2)
Fig.2. Features of the spread of pigmented spots in fissures.
The absence of a carious cavity is explained by the anatomical shape of the fissures themselves, in which the carious process spreads initially deep into the enamel and dentin, and then a defect in the form of a cavity is formed.On this basis, I believe it is inappropriate to pay special attention to the absence of a visible carious defect, especially since the final diagnosis of such cavities is unambiguously made only after the opening and treatment of the carious cavity.
In addition, the WHO classification considers not only one form of dentin caries, but also one form of cement caries.At the same time, this form of caries with lesions of cement and root dentin is characterized by various types of carious cavities with a diverse combination of zones of the carious process, as a result of which the clinic and treatment of these root lesions have their own characteristics.Based on this, it is necessary to supplement the carious lesions of cement with appropriate forms, especially since the treatment of some root lesions is still problematic (see below)?
It is also important to note that Prof. P.A.Leus in his article "Improving the classifications of dental caries and their importance in the practice of a dentist" writes that in practice diagnoses with codes K02.4,K02.8,K02.9 are not actually used. In addition, the gap between the WHO classification is not clear nosologies K02.4 and K02.8 .
I would also like to touch upon the international system for the determination of dental caries (ICDAS), which integrates several classifications of caries, using a 6-digit scale to indicate lesions from initial manifestations to extensive carious cavities, and also assesses the activity of caries on an additional 2-digit scale.
Unfortunately, this classification is not without its drawbacks.First of all, this refers to the allocation of too many forms of enamel damage (actually 4). If we take into account the rather insignificant thickness of the enamel, it is almost impossible to differentiate these numerous enamel lesions, especially lesions similar to superficial caries (see above).As for the two dentin lesion codes (5 and 6), there is nothing new here either, since these are actually medium and deep caries.
Based on the above, I propose a clinical classification of caries, which takes into account all the above disadvantages of existing classifications :
Dental caries
Enamel caries
•The stage of the "white spot" ( initial clinical manifestation of caries)
•The stage of "pigmented spot" (arrested
enamel caries)
Caries of crown dentin
• Dentin caries
• Progressive dentin caries
• Arrested dentin caries
Caries of cementum and root dentin
• Cement caries
• Progressive cement caries
• Arrested cementum caries
I believe that a detailed designation in the classification of the affected tooth tissues is more informative, although the usual designation can be used: enamel caries, dentin caries and cementum caries.
Based on the above, a tooth crown is considered healthy if there are no traces of initial clinical manifestations of caries (white spot), visible carious enamel demineralization (pigmented spot) and carious demineralization or carious defect affecting the crown and root dentin.
Let's take a closer look at the proposed caries nosologies in the new clinical caries classification.
Enamel caries
White spot stage (initial clinical manifestation of caries)
The initial clinical manifestation of enamel caries is a white spot.Clinically, this stage is manifested by the loss of the natural color and gloss of the enamel, with the formation of a white or light yellow spot on the enamel surface (Fig.3).It is important to note that at this stage of the carious process through the disintegrated enamel prisms from the bacterial plaque can diffuse acids, but not the microorganisms themselves. And only after the destruction of enamel begins microbial invasion into the dentinal tubules. This form of caries is characterized by subsurface enamel demineralization.Caries in the stain stage is mostly asymptomatic and is detected only upon careful examination, because there is no enamel defect at this stage.
Fig. 3. “White spot” stage.
To identify carious spots, it is recommended to remove plaque from the surface of the stain and dry the crown of the tooth, while the intact enamel retains its shine, while the surface of the carious spot becomes matte. Curiously, G. V. Black (1908) was the first to draw attention to this phenomenon, who noticed that when drying the tooth surface, air replaces water in a carious lesion through the pores of demineralized tissue.And since the refractive index of air is less than that of water, the lesion becomes visible when dried.
Patients mostly complain of the appearance of a white or light yellow spot.When probing, roughness, slight pliability and soreness may be noted.An effective method of diagnosing white spot is the use of color reactions with various dyes.When white spots are located in the fissures, there may be difficulties in their diagnosis, which is due to their intense pigmentation in the fissures, where food residues and pigments are more likely to accumulate.Therefore, white carious spots are practically not diagnosed in the fissures, which has an important clinical significance.
Treatment of white spots is aimed at restoring the affected tooth enamel surface by remineralizing therapy.
The stage of "pigmented spot" (аrrested enamel caries)
With the prolonged development of the pathological process, due to the penetration of pigments from food, tobacco, and pigment-forming microflora into demineralized tissues, the white spot undergoes transformation and can turn into a pigmented spot.This form of enamel caries is characterized by light brown, dark brown and black spots, the removal of which does not disrupt the enamel-dentine connection (Fig.4).
Fig. 4. Pigmented spots.
Pain is not observed, although sometimes there may be a slight pain in the tooth.Patients mostly complain of a cosmetic defect due to the appearance of dark spots.Moreover, the carious process due to mineralization may not progress for a long time.That is why this form of pigmented spot is considered a аrrested enamel caries.
Moreover, Pakhomov believed that only dark brown and black spots are characterized by damage to the enamel-dentine border, while light brown ones are without damage to the enamel-dentine border.However, Professor Borovsky has convincingly proved that dark brown and black spots are often diagnosed in the clinic without damage to the enamel-dentine border.
Thus, a pigmented spot as a arrested caries can be located only within the enamel, and when the carious process progresses to dentin, it turns into dentin caries. A pigmented spot is a spot because it is not characterized by the lesion of the enamel-dentin border, and that is why it is actually a transitional form between enamel and dentin caries!
In the treatment of a pigmented spot, it is sufficient to remove pigmentation on smooth surfaces and carry out remineralizing therapy.If the fissures are affected, their invasive sealing can be carried out, and if the enamel – dentine joint is slightly affected, then extended sealing of the fissures is acceptable (Fig.5).
A B V
Fig.5. Fissure sealing techniques (E. Helwig, 1999).
А. Non-invasive fissure sealing.
B. Invasive fissure sealing.
V. Extended fissure sealing.
It should be noted that non-invasive fissure sealing is a purely prophylactic procedure and is performed in teeth that are not affected by caries.
Caries of crown dentin
Dentin caries
With progression, the white spot may directly transform into dentinal caries, but more often in the clinic it is transformed into a pigmented spot, which eventually spreads to the dentin, becoming dentinal caries.Due to the structural features of the structure of dentin, the course of the carious process in it has its own characteristics and occurs more actively than in enamel.
In this form of dentin caries, a carious cavity with a narrow and sometimes wide entrance opening is objectively revealed in fissures and on smooth enamel surfaces.The carious cavity is filled with food residues and softened pigmented dentin from yellow-brown to brown and black.
Patients with this form of dentin caries may complain of pain, food sticking, or a cosmetic defect.Pain arises from thermal, mechanical and chemical stimuli and disappears immediately after their elimination.Sometimes there may be no pain at all.Probing the bottom and walls of the carious cavity may not always be painful, depending on the depth of the lesion..Radiologically, there are no changes in the tissues surrounding the root of the tooth.The above data allow us to make only a preliminary diagnosis.
The final diagnosis is made after the preparation of the carious cavity.As a result of the removal of decayed pathological tissues, we obtain a prepared cavity with dense walls within the mantle dentin or periculpar dentin.Pain is observed during preparation and probing of the cavity, although pain may be absent during the formation of sclerosed and replacement dentin (Fig.6).
Fig.6. Prepared and sealed carious cavities with dentin caries.
An important guideline in the diagnosis of dentine caries is not so much the depth of the lesion (the distance from the surface of the tooth to the bottom of the carious cavity), but the condition of the bottom of the prepared cavity (dentine bridge).The latter in the prepared cavity of dentine caries is dense without signs of demineralization, and sometimes with a certain degree of mineralization.Such a condition of the bottom of the prepared cavity is associated with the formation of protective and adaptive zones of the carious process (sclerosed and replacement dentin), which reliably protect the tooth pulp from damage and guarantee success in adequate treatment.
Therefore, in the treatment of this form of dentin caries, it is sufficient to remove demineralized tissues and seal the tooth without the use of therapeutic and insulating pads.
Progressive dentin caries
In this form of dentin caries, softened dentin from gray-yellow to black is found in the carious cavity, affecting the entire thickness of the periculpar dentin.When probing, soreness is noted along the walls and bottom of the carious cavity, especially at the points closest to the pulp of the tooth.
Patients complain of a cosmetic defect, food jamming, sharp pain resulting from the action of thermal, mechanical, chemical stimuli, disappearing immediately after their elimination (Fig.7).Radiologically, there are no special changes in the tissues surrounding the root of the tooth.These data make it possible to make only a preliminary diagnosis, and the final diagnosis is made only after preparation of the carious cavity .
Fig.7.Progressive dentin caries.
As a result of the removal of decayed tissues, we obtain a prepared cavity within the parapulpal dentin.Preparation and probing of this cavity is sharply painful.The walls of this cavity are dense, while the bottom of the prepared cavity (dentine bridge) is quite thin and elastic, and sometimes with signs of pigmentation.In some cases, the pulp is slightly translucent through the thinned bottom of the cavity.
Probing the bottom of the prepared cavity and removing demineralized softened dentin from the bottom of the cavity must be carried out very carefully, since at the projection points of the pulp horns the arch of the tooth cavity is very thin, therefore it is easy to pierce it with a probe, opening the tooth pulp, which is accompanied by sharp pain and the appearance of blood droplets in the carious cavity.As a result, such a pathology can no longer be considered caries and should be diagnosed in the section "pulpitis".This clinical picture is associated with the lack of formation of protective and adaptive layers of the carious process in the tooth (sclerosed and replacement dentin).
This is the most unfavorable and unpredictable form of dentin caries both in terms of diagnosis and treatment, since it is impossible to accurately determine the type and degree of inflammation of the pulp and the possibility of its further functioning!That is why in different countries such a pathology is attributed to caries or initial pulpitis. For example, the progressive form of caries in Russia is referred to as deep caries. The American Dental Association (ADA), oddly enough, considers progressive caries (also called endodontic caries or root canal caries) to be a form of caries that spreads to the pulp chamber and even to the root canal system.And only the WHO classifies such a pathology as an initial pulpitis.
In this regard, statements about such carious lesions with an unopened pulp chamber by scientists M. Bushan and V.Kulazhenko deserve attention, who in the book "Dental caries, its treatment and prevention using vacuum electrophoresis" (1975) unequivocally stated that this condition is actually a transitional form between caries and pulpitis and is diagnosed as deep caries with hyperemia phenomena.
Regarding the transitional form, of course, one can agree, however, with such a pronounced pathological decay of dentin, it is difficult to agree on pulp hyperemia, which is the initial form of pulp inflammation that developed in the early stages of the development of the carious process.As is known, inflammation in the pulp occurs immediately as soon as the carious process affects the tooth enamel (Simon, 1972).At this stage of the development of the carious process, lymphocytes can be detected that are not detected in the non-inflamed intact pulp.Moreover, bacterial toxins, enzymes, and antigens enter the pulp earlier than the bacteria themselves (Trowbridge, 1972).Such inflammation is considered to be initial (hyperemia), which differs significantly from severe inflammation of the pulp, when bacteria directly penetrate into the pulp of the tooth.
In essence, pulp hyperemia is one of the protective stages of the inflammatory-reparative process and is found not only in caries, but also in the preparation of the carious cavity, pathological erasability, various periodontal diseases, etc. Consequently, hyperemia is not a nosology, but only a symptom found in various diseases, as a result of which it makes no sense to single it out in the WHO classification of pulpitis.It was precisely this mechanism of protection against infection that Seltzer considered the initial inflammation, which he called "pulp hyperemia" and considered a transitional stage from the initial inflammatory process to advanced pulp inflammation.
In this case, chronic forms of pulp inflammation clearly prevail, which is indirectly evidenced by: a long-term carious process with pathological destruction of periculpar dentin, absence of pain (chronic course), absence of protective and adaptive layers of the carious process (sclerosed and replacement dentin). After all, that is why it is difficult to preserve such an inflamed pulp by a biological treatment method, while with normal hyperemia there is no need to use therapeutic pads at all.
Unfortunately, without morphological studies, which are not carried out in the clinic, it is impossible to accurately determine the condition of the pulp and even more so to determine the moment of transition of hyperemia into pronounced inflammation of the pulp.In addition, it is impossible to establish a correlation between clinical manifestations and morphological data of the pulp. Attempts to link the nature of pain with the condition of the pulp were unsuccessful, because, according to Simon, there is no correlation between the severity of pain and the degree of damage to the pulp.
That is why clinicians V.S. Ivanov and L.I. Urbanovich quite reasonably argued that the biological method is discredited not because it is not possible to keep the pulp viable, but because it is impossible to accurately identify the degree and stage of pulp inflammation. In addition, in this case, the emphasis should be placed not on the alleged reverse transformation of pulpitis into caries (reversible pulpitis), but, conversely, on the possibility of preventing the progressive transformation of caries into advanced pulpitis.
Also noteworthy is the debate about the appropriateness of moving
the nosology “progressive dentin caries” in the section “pulp inflammation” in the WHO classification of pulpitis, with which it is clearly difficult to agree. In this regard, the interpretation of the nosology “initial pulpitis” or “pulp hyperemia” in the WHO classification is the most controversial, since this form includes diseases that are different in clinical and morphological data, and for the treatment of which, in addition, completely different techniques are used (direct and indirect coverage).
In the WHO classification, the nosology of “initial pulpitis”, in the treatment of which direct pulp coverage is performed, should unambiguously include only those forms of initial pulpitis in which there was an accidental opening of the pulp cavity during trauma to an intact tooth or during the treatment of dense and uninfected layers of mantle dentin in the treatment of, for example, shallow dentin caries.In this case, it is indeed the initial inflammation of the pulp, because the pulp was not directly infected by microorganisms before opening. If it is possible to prevent the penetration of microorganisms into the pulp of the tooth in time by direct covering of the pulp with therapeutic pads, it is possible to save the pulp.
At the same time, if there was a perforation of the pulp cavity during the evacuation of fully softened infected parapulpal dentin, it is not recommended to perform direct pulp coverage, because in this case we have not the initial inflammation of the pulp in the form of hyperemia, but already irreversible developed inflammation of the pulp.
Indirect coating of the pulp is carried out only with an unopened pulp cavity, when the softened infected parapulpal dentin is maximally removed and the tooth pulp is separated from the bottom of the prepared cavity by a thin dense layer of parapulpal dentin (dentine bridge), sometimes with signs of partial demineralization. In this case, it is illogical to diagnose initial pulpitis or pulp hyperemia, since once sclerosed and replacement dentin has not been formed, then microorganisms and toxic products of their vital activity have definitely already penetrated into the tooth pulp from infected parapulpal dentin, as a result of which the pulp is susceptible not to initial, but already developed inflammation.That is why therapeutic pads (indirect coating) are used to eliminate the inflammatory process in the pulp.
In case of successful exposure of the material of therapeutic pads to the inflamed pulp, the deposition of sclerosed and replacement dentin (tertiary dentin) occurs, which prevents further infection of the pulp.However, during the deposition of replacement dentin on the walls of the pulp cavity, the pulp volume decreases, the collagen part increases and the cellular composition decreases, resulting in a decrease in its functions.This condition is called "pulp atrophy" and it is in this condition that the pulp functions in a biologically cured tooth (Fig.8).
Fig.8.Protective and adaptive layers of carious process that caused pulp atrophy.
Thus, the inflamed pulp never returns to its original non-inflamed state, however, in a state of pulp atrophy, it can function for a long time in a cured carious tooth.Based on this, since it was possible to prevent the progression of the developed inflammation, it is logical to attribute this nosology to caries (progressive dentine caries), and not to the initial pulpitis.By the way, the first material for the therapeutic coating of the bottom of the carious cavity was gold.This technique was first described in 1756 by the personal dentist of the Prussian king Philip Pfaff.
Thus, a rather paradoxical situation arises when, in the WHO classification of pulpitis, pathology with initial inflammation of the pulp (hyperemia), for which direct coating is used, and pathology with clearly developed inflammation of the pulp, for which indirect coating is used, are attributed to the same nosology "initial pulpitis".
In this case, nosology, in which direct coating is carried out, is certainly correctly attributed to initial pulpitis, but nosology, which is characterized by already developed inflammation of the pulp and for the treatment of which indirect coating is carried out, it is illogical to refer to initial pulpitis.The logical question then arises - to which nosology (caries or pulpitis) should this unpredictable pathology be attributed from the point of view of treatment? Unambiguously unpredictable, since it is impossible to accurately predict whether, as a result of indirect pulp coating, it will be possible to prevent the transformation of caries into developed pulpitis.
That is why in this case it is necessary to make a long-term preliminary diagnosis (this concept is found for the first time in the scientific literature), and not a final diagnosis.Since the main therapeutic actions are aimed at treating caries that caused inflammation of the pulp,it is more logical to first diagnose "progressive dentine caries".If, after indirect coating of the pulp and applying a temporary seal for some time (several weeks), the patient's complaints completely disappear and there is no exacerbation of the process, then it will be possible to make a final diagnosis of "progressive dentine caries" and seal the tooth.If during this time it is not possible to prevent the transformation of caries into pulpitis and an exacerbation of the process occurs, then this nosology should be attributed to one of the forms of developed pulpitis, and not to caries, and even more so not to initial pulpitis.
Thus, in the diagnosis of progressive caries, one of the most important factors is to determine the reversibility or irreversibility of inflammation in pulp tissues, since this parameter is the key moment both in diagnosis and in choosing a treatment method, and not the fact of the developed inflammation itself. In this regard, the research of Levin L.G. deserves attention, which found that pulpitis usually becomes irreversible when the pulp has pronounced inflammation with signs of necrosis, which makes it impossible to use a biological treatment method.
Unambiguously, such a progressive carious pathology with an unopened pulp chamber, which is difficult to diagnose before determining the outcome of treatment with indirect pulp coating, is at first more logically attributed to carious pathology rather than pulpar. In this case, it is also illogical to attribute it to other forms of advanced pulpitis, since none of them carries out a biological method of preserving pulp.
It is also illogical to attribute this pathology to reversible pulpitis, mistakenly assuming the transformation of pulpitis into caries.Based on all of the above, it is undoubtedly advisable to consider this carious pathology, in which it was possible to prevent the complete transformation of caries into pulpitis, a transitional form between caries and pulpitis. In the case of a negative outcome of treatment, based on the clinic of progressive pulpitis, this pathology can easily be attributed to one of the forms of advanced pulpitis.
I will say more, the transformation of caries into pulpitis is sometimes prevented by nature itself even before the treatment of progressive caries as a result of the formation of sclerosed and replacement dentin by the protective forces of the body, preventing the penetration of microbes and products of their vital activity from the decayed and infected peri-pulp dentin into the pulp of the tooth. After all, that is why it is illogical to diagnose such a form of caries, in which nature itself has prevented the transformation of caries into pulpitis, as “initial pulpitis” and use medicinal pads.
Thus, it is advisable to consider progressive dentine caries as a transitional form between caries and pulpitis.This approach is also justified by the fact that it becomes possible to justify the legal responsibility of a doctor in the treatment of this neglected form of caries, since by fixing such a diagnosis and warning the patient in advance about possible complications, the doctor, in case of an exacerbation of the process, relieves himself of legal responsibility, unless, of course, adequate treatment has been carried out.
In this case, with the consent of the patient, the doctor, taking into account the body's defenses, did everything possible to prevent the complete transformation of caries into pulpitis.If the diagnosis of such a pathology is shifted towards pulpitis, then in case of an exacerbation of the process, it will undoubtedly be more difficult for the doctor to justify himself, since, pointing to the nosology "pulpitis" in the diagnosis, he did not carry out the only reliable method of treating this pathology – extirpation of the pulp.
In this regard, how prophetic was the tactics of Russian scientists, who, unlike the creators of the WHO classification, half a century ago quite reasonably proposed to take into account the transitional form between caries and pulpitis, referring this nosology to deep caries, and not to the initial pulpitis, as it is still proposed in the WHO classification of pulpitis.
Arrested dentine caries
With sufficient resistance of the body and other favorable conditions, the carious process in dentin, as in enamel, may proceed more slowly or even completely stop.In such cases, it is called arrested or stationary caries. More often, such a course of caries is noted on the occlusal surfaces of teeth, which are subjected to abrasion during chewing, as a result of which the carious defect, subjected to such an action, is completely remineralized (Fig. 9).Such dynamics of the course of the carious process is especially characteristic of carious lesions with a predominance of mineralization processes over demineralization.
Fig.9.Аrrested dentin caries on the abraded cheing surface of a molar.
Any form of dentin caries can turn into stationary caries, which is most often the outcome of a chronic course, although cases of direct transition to this form of an acute course of the carious process have been described.The initial and subsequent stages, depending on the depth of the stationary carious process, are characterized by the appearance of intense brown, black-brown color of dentin in the affected area. In this form of caries, a peculiar mineralized "scar" can be found on the hard tissues of the tooth, indicating a carious lesion in the past. Sometimes tooth tissues, due to increased remineralization, become vitreous, as a result of which this form of caries is also called "sclerosed caries".
Defects in the hard tissues of the tooth due to the erasure of occlusal surfaces during chewing have wide entrance openings, an open saucer shape.In deep carious cavities, their bottom may be within the boundaries of the secondary dentin, i.e. above the level of the arch of the tooth cavity (Fig. 10). Due to this course of the carious process, the pulp manages to form a significant layer of replacement dentin, which differs significantly in its mineralization from the replacement dentin formed in ordinary dentin caries.
Fig.10.Arrested dentin caries in a deep carious cavity of a premolar.
In this form of caries, due to the high mineralization of enamel and dentin, even in the deep carious cavity, pain is not observed.Patients turn to the dentist mainly with complaints of a cosmetic defect and for fear of losing a tooth.
It is important that the fixation of composite materials in this form of caries is extremely difficult, since the use of adhesive systems due to the high mineralization of the affected tooth tissues is ineffective, unlike conventional forms of dentin caries.Therefore, it is preferable to use glass ionomer cements that form a chemical bond with tooth tissues or use a sandwich technique, and sometimes it is more advisable to cover such teeth with appropriate orthopedic crowns.
At the same time, it is necessary to take into account that with high mineralization of the affected tissues, new carious foci do not occur in areas of highly mineralized stationary caries, but on intact tooth surfaces, which is already a mandatory reason for restoration.
At the same time, such forms of caries cannot be considered ordinary dentine caries with a layer of replacement dentine formed and not be singled out separately in the classification as arrested dentine caries.
Caries of cementum and root dentin
Cement caries
Cement caries most often occurs in the cervical area of the exposed surface of the root (Fig. 11).Root cement is more vulnerable to the demineralization process than enamel.In addition, the roots of the teeth have a very thin layer of cement, which contributes to a faster progression of the carious process into the root dentin, the structure of which is somewhat different from the crown dentin (root dentin contains fewer dentine tubules than the crown).Carious lesions in the root area often spread both to the crown of the tooth and circularly around the root (circular caries of cement).
Fig.11.Cement caries.
Patients with this form of caries complain of pain resulting from thermal, mechanical, and chemical stimuli that disappear immediately after their elimination.Objectively, after the removal of decayed tooth tissues, a carious cavity in the root part of the tooth is diagnosed with damage to the middle layers of the root dentin.In general, the clinical manifestations and tactics of treatment of root caries are the same as in the crown of the tooth, especially since these lesions are often combined.
Cement caries occurs mainly in patients over 60 years of age.Its occurrence is associated with poor oral hygiene in old age, the presence of areas of exposure of the root surface in pаrodontitis, decreased saliva secretion, taking medications, etc. Cement caries develops especially intensively in people who have undergone radiation therapy in the head and neck area.It is important to note that cement caries is initiated not by Str. mutans, but by Actinomyces viscus and its transformation occurs without the "white spot" stage.
In addition, in the root cement in the early stages of the lesion, preventive measures may prevent its progression. To do this, on the recommendation of the German scientist E. Delvig, it is enough to remove a demineralized section of cement with an excavator or a spherical boron, and then carry out several applications with a fluoride-containing varnish or gel (remineralizing therapy). On this basis, in the proposed clinical classification, at the request of clinicians, it is also possible to identify the initial clinical lesion of cement caries (caries of the cement surface). By the way, in the 1995 WHO classification, this form of cement caries was initially distinguished, but later, for some reason, this tactic was abandoned.
With a significant lesion of cement and root dentin, operative restorative treatment is carried out, which also has its own characteristics associated with the problematic binding of adhesive systems and composites with tooth cement.In addition, when filling caries with cement that spreads to the crown of the tooth, it is necessary to simultaneously create conditions for adhesion to enamel, cement, crown and root dentin, which is extremely difficult.Based on the above, the treatment of such root lesions is sometimes still problematic.
Progressive cement caries
Patients with this form of cement caries complain of pain resulting from thermal, mechanical, and chemical stimuli that disappear immediately after their elimination. Objectively, after the removal of decayed tooth tissues, a carious cavity in the root part of the tooth is diagnosed with damage to the deep layers of root dentin, as a result of which an indirect coating of the pulp is applied. In general, the clinical manifestations and tactics of treatment of progressive root caries are the same as in the crown of the tooth, especially since these lesions are often combined.
Curiously, the progression of caries in the root dentin is easier to stop than in the crown dentin, since the reparative-restorative processes in the root dentin are more pronounced.
Arrested cementum caries
It is known that in periodontal diseases, root dentin reacts to the influence of stimuli by increased formation of sclerosed and replacement dentin, which significantly slow down the development of caries. Therefore, I think it is logical to highlight arrested cementum caries in the clinic (Fig.12).
Figure 12.Arrested cementum caries.
The clinic and principles of treatment of this form of cement caries are similar to arrested dentine caries, especially since these lesions are often combined.
Caries is the most common and diverse pathology in the human body, therefore, it is not enough to classify caries using only clinical classification. Based on this, the accepted multi-system classification of caries is fully justified: by localization, by the nature and dynamics of the course, by the intensity of the lesion, by the sequence of the process, the allocation of special forms of caries, etc.. It is also important to take into account infant caries, childhood caries and adolescent caries separately.
In this regard, attention should be paid to bottle caries, a disease of young children that occurs as a result of children's habit of drinking milk formula from a bottle before going to bed, as a result of which lactose residues accumulate in the oral cavity, which is a breeding ground for bacteria.
Moreover, not all of these classifications need to be used in the clinic for the diagnosis of caries, since some of them are of purely scientific importance.For example, there is no strict need to distinguish acute and chronic caries in the clinic during diagnosis, since caries, in principle, is a chronic pathology.
In this regard, it is necessary to agree with Professor E. V. Borovsky, who in the book "Dental caries: preparation and filling" (2001) believes that such a division in the clinic is unauthorized, since even with an intensive carious process, at least 3-6 months pass from the moment of demineralization to the moment of formation of the carious cavity, which does not it fits into the framework of the development of an acute process accepted in medicine.
The exception is a rare and special form of caries with partial or complete damage to the salivary glands (acute caries), which occurs for 2-5 weeks, as well as a clinical variant of acute caries with multiple dental lesions flowering caries (caries florida).Clearly, these forms of caries are characterized by an acute course.In addition, by highlighting the progressive and suspended course of caries in the proposed clinical classification, clinicians can indirectly judge the acute and chronic course of this pathology.
At the same time, when making a diagnosis based on the proposed clinical classification, for a more accurate and detailed diagnosis, it is desirable to use a comprehensive diagnosis of caries, which will display various characteristics of the carious process that directly affect the choice of treatment tactics.
First of all, this refers to the localization of the carious process on the surface of the tooth (fissure, contact, cervical, circular caries), which sometimes directly affects the treatment tactics. As is known, due to the complex configuration of the tooth crown with different directions of the enamel prisms, the spread of caries on different tooth surfaces has a number of features.
In this regard, the classification of the localization of carious lesions according to Black needs to be revised and modernized, since it is not without drawbacks and no longer meets the modern requirements of clinicians (read more about this in my article (https://dzen.ru/a/ZF8unVI3ImYrqWYp ).That is why ADA, with its CCS system, primarily due to the inability to recognize the earliest signs of the lesion, and thereby underestimate the prevalence and severity of the disease, tries to correct the shortcomings of the Black system.
In addition, the tactics of formation of carious lesions are clearly influenced not only by their localization, but also by belonging to isolated or combined cavities (Fig. 13.).Isolated – cavities located on one or more tooth surfaces that do not connect to each other. And when several carious cavities on different surfaces of the tooth connect to each other, then we are talking about combined cavities. Such a separation of cavities is essential for the tactics of the formation of a carious cavity, since in combined cavities, after preparation, the main and additional sites are often isolated.
Fig.13. Isolated (a) and combined (b) carious cavities.
Moreover, it is advisable to classify combined carious cavities as follows:
l. Carious cavities on the chewing or cutting surface with a diverse combination of adjacent surfaces involved;
2. Carious cavities on the proximal surfaces with a diverse combination of involved lingual and labial surfaces;
3. Extensive carious cavities with the absence of one or more tooth surfaces.
Thus, in the classification of the localization of carious lesions, in order to take into account the full variety of carious lesions, instead of the Black classification, it is enough to separately identify isolated cavities (fissured, contact, cervical, circular caries) and the system of combined lesions proposed by me.
It is also important to take into account the primary and secondary occurrence of the carious process in the clinic.Primary caries is the occurrence of a process in an intact tooth.The occurrence of a carious process in a tooth already affected by caries should be considered secondary and recurrent caries.Unfortunately, the interpretation of secondary and recurrent caries varies in different dental schools and is not always scientifically justified.
That is why I would like to offer my own interpretation of these forms of caries.Recurrent caries should be considered the resumption of the carious process at the boundaries of the previously placed filling as a result of poor-quality preparation of the carious cavity, polymerization shrinkage of the filling material, as well as other errors made during filling of the cavity.
And secondary caries should be considered the occurrence of a carious process in a tooth already affected by caries, outside the boundaries of a previously placed seal (Fig.14). You can read more about this in my monograph "Modern cariesology".
Fig.14. Recurrent caries (a), secondary caries (b, c).
It is also important to note that as a result of excessive fluoridation of enamel during preventive measures, the carious process in dentin often occurs without damaging the integrity of the enamel. A similar form of dentine caries can only be detected by X-ray examination, where such hidden cavities are defined as areas of enlightenment in the dentine (hidden dentine caries). It is with this pathology that patients often complain of increased sensitivity in their teeth without revealing carious lesions. At the discretion of clinicians, this form of caries can also be distinguished in the classification of dentin caries or simply attributed to atypical or special forms of caries (Fig.15).
Fig.15. Hidden (atypical) dentin caries (A.I. Nikolaev, L.M. Tsepov, 2001).
Based on the above, a comprehensive diagnosis of caries, for example, can look like this:
Secondary,isolated,fissured,dental caries of the 14th tooth;
Primary,combined,contact,cervical arrested dental caries of the dentin of the 15th tooth;
Recurrent, circular, progressive caries of the cement of the 26th tooth;
Acute, combined,occlusive, contact,progressive dental caries of the 27th tooth.
A wide variety of combinations of a comprehensive diagnosis of caries are possible (this is the topic of a separate article). This tactic of making a comprehensive diagnosis of caries allows you to take into account all the variety of forms of manifestation of the carious process. At the same time, it is more informative, and also makes it possible to simplify the description of the objective picture of the carious process.
CONCLUSIONS
Dear colleagues, I hope you will like the proposed clinical classification and the use of a comprehensive diagnosis of caries, since the proposed nosologies are the main forms of manifestation of the carious process in tooth tissues. In addition, they are quite easily diagnosed in the clinic, which cannot be said about some nosologies in various classifications of caries, the diagnosis of which is difficult, and sometimes even impossible, such as, for example, the diagnosis of superficial caries.
In conclusion, I invite clinicians and all interested parties to participate in the discussion of the new version of the clinical classification of dental caries and the possibility of its use in clinical practice.
I will gratefully accept and take into account all amendments and recommendations sent by you (otari@inbox.ru).
Conflict of interests. The author declare no conflict of interests.
Otari Eduardovich Khidirbegishvili is a graduate of the SSMI in 1978, who has been engaged in practical, scientific and pedagogical activities in the city of Tbilisi for more than forty years. During this time, more than 100 articles have been published in leading dental journals, and in 2005 the Dental Association of Russia published a monograph "Modern Cariesology", which is accepted for teaching in Russia and in many countries. Due to developments in the field of theoretical dentistry, the photo is placed on the cover of the Russian magazine "Maestro of Dentistry" (№ 1(10)2003).
REFERENCES
1. Borovsky E.V. Terminology and classification of dental caries and its complications // Clinical dentistry. - 2001. - No. 1. - pp.10-12. / Borovsky E.V. Terminology and classification of dental caries and its complications. Clinical Dentistry, 2001, vol. 1, pp.10-12.
2. Leus P.A. Classification of Caries by the name of a person: from G.Black books // Mathematical Journal. – 2015. – Vol.16, No.1. – pp.6-15. / human dental caries: from G.Black to CLASS [Classification of human caresses death: from G.Black to ICDAS. Dental Journal, 2015, vol. 16, No.1, pp.6-15. (in Russian)
3. Pakhomov G.N. Dental caries and its prevention. – Riga: Publishing house "Dentistry", 1976. – 128 p. / Pakhomov G.N. Dental caries and its prevention. Riga: Publishing house "Zinatne", 1976, 128 p.
4. Bushan M.G., Kodola N. A. Dental caries. Goskomizdat–.1975.-p. 114.
5. Khidirbegishvili O. E. Modern cariesology. – Moscow:Medical Book, 2006 - p. 134.
6. Helvig E., Klimek J., Attin T. Therapeutic dentistry. – Lviv: GalDent, 1999.-pp. 155, 30.
7. International Classification of Dental Diseases ICD-DA, WHO, Geneva, 1995.
8. Borisenko A.V. Dental caries. Kiev: Book plus.-2000.-p. 120. 12.
9. Seltzer S. Bender J.R. The Dental Pulp. Considerations in Dental Procedures. – Philadelphia, P. A. US Zippincot 1984
10. Braga M.M., Oliveira L.B., et al. Feasibility of the international caries detection and assessment system II in epidemiological surveys and comparability with standard WHO criteria. Caries Research, 2009, vol.43, pp.245–249.
11. Bratthall D. The Significant Caries Index. International Dental Journal, 2000, vol.50, pp.378–384.
12. Fejerskov O., Kidd E.A.M. Dental caries. Blackwell Munksgaard, 2004, 560 p.