Khidirbegishvili O.E.
Dentist. Tbilisi, Georgia
Abstract The article presents scientific data on the modernization of pulpitis classification. It describes the shortcomings of existing classifications, including the WHO classification, proposes new nosological forms, and formulates principles for constructing a modern classification of pulpitis. The proposed classification allows for the consideration of numerous forms of pulp pathology and is more convenient for use in clinical practice.Using the proposed classification, it is possible to make scientifically based diagnoses of pulpitis.
Keywords:classification of pulpitis, pulpitis, pulp hyperemia, pulp necrosis, pulp degeneration, pulp atrophy.
For citation:O.Е. Khidirbegishvili .Modernized classification of diseases and conditions of the pulp.Stomatology for All / Int. Dental Review.
Introduction
One of the first attempts to systematize inflammatory processes in the pulp were the classifications of pulpitis by Linder (1851) and Arkevi (1886).Since then, many different variants of their construction have been proposed, but it has not yet been possible to create a generally accepted classification of pulpitis that meets the requirements of clinicians. In general, according to Prof. Petrikas A.Yu., pulpitis can “boast” of the number of proposed classifications.
I would like to share my opinion on the classifications used and propose a clinical classification of pulpitis that meets the requirements of clinicians and is convenient for use in clinical practice.
Material and methods
The complexity of creating a unified clinical classification of pulpitis is associated with imperfect diagnostic methods and the lack of correlation between the clinical manifestations of this pathology and the data of histological studies, which are not conducted in clinics, making it difficult to determine the resistance status of pulp pathology. This is why it has not yet been possible to create a universally accepted classification of pulpitis. Unfortunately, the WHO classification of pulpitis is no exception [1].
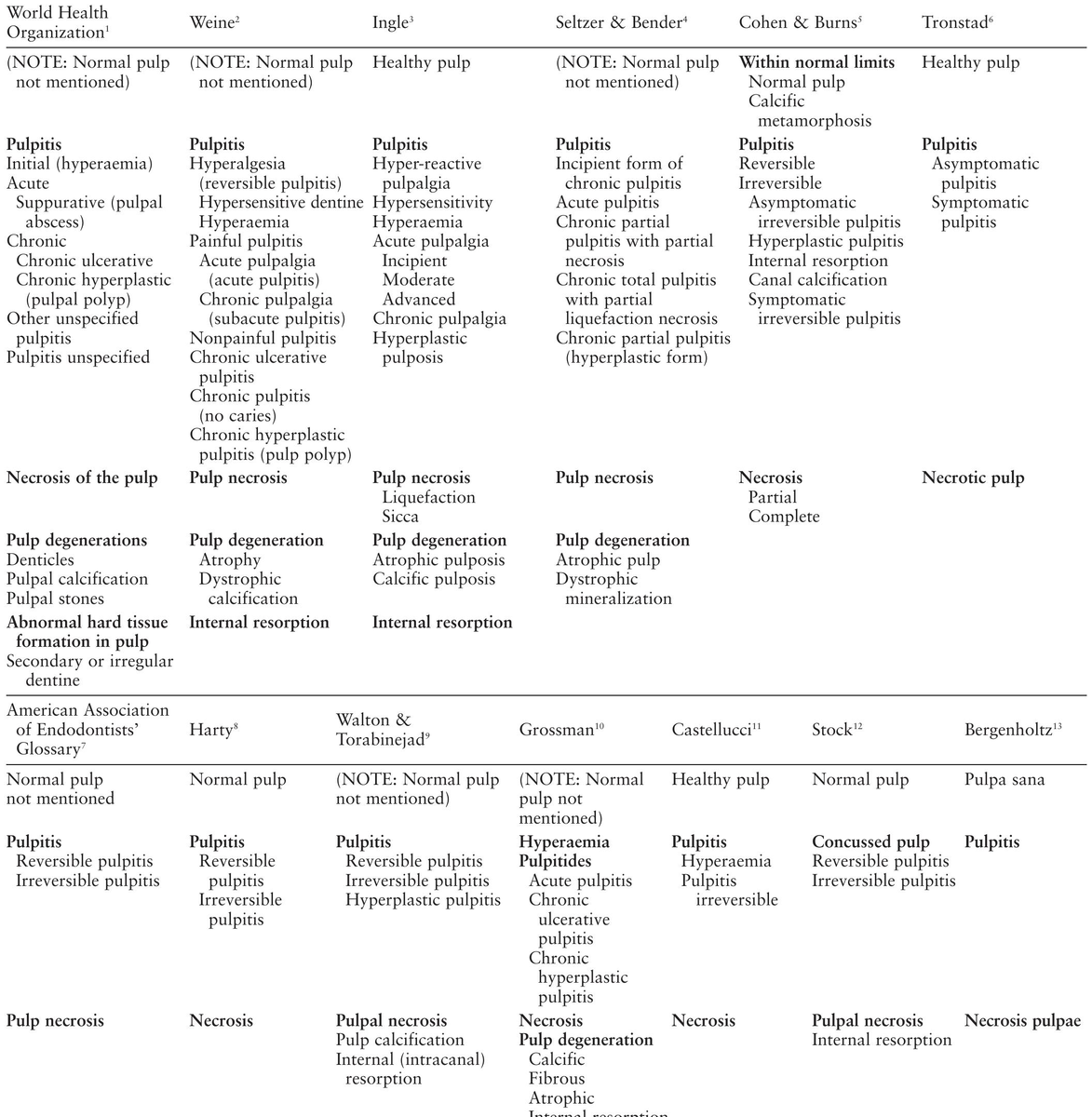
When considering the classifications used in different countries, one is amazed at how different and contradictory they are, and sometimes even gets the impression that we live on different planets. For example, American and European scientists use the classifications presented in the (Table 1), which focuses on pulp hyperemia, reversible and irreversible pulpitis, symptomatic and asymptomatic pulpitis, etc..
Table 1.
In Russia and post-Soviet countries, classifications of pulpitis are still used, in which the main emphasis is placed on serous and purulent inflammation, acute and chronic, as well as exacerbated inflammation of the pulp, etc. [2]. Paradoxically, these types of inflammatory process in the pulp are difficult to diagnose, and sometimes they are completely impossible to diagnose.For example, serous inflammation of the pulp is the initial stage of acute pulpitis, after which the serous exudate turns into purulent. However, this transformation occurs so quickly that it is impossible to trace it not only by clinical, but sometimes also by morphological research methods [2].Since the symptoms of serous and purulent pulpitis are difficult to differentiate, and their treatment is, in principle, the same, there is no point in distinguishing these two forms of pulp inflammation in the classification.
In addition, in the classification of pulpitis, it is inappropriate to separately distinguish acute, chronic and exacerbated chronic pulpitis, without taking into account the specifics of the course of these processes, since most such pathologies do not actually arise acutely initially (the only exception is traumatic injuries).Clearly, at first the symptoms of most diseases develop unnoticed by the patient (chronic course),and then an acute course occurs as a result of an exacerbation of a chronic process, which can again become chronic.
Thus, an acute process is basically an exacerbation of a chronic process, so there is no point in differentiating these processes in the classification. That is why, for example, an exacerbation of a process is quite justifiably not distinguished in the WHO and AAE classifications, as well as in many classifications used [1][3].
At the same time, it is necessary to clearly understand that the terms “acute” and “chronic” should be used in the classification simply as indicators of the patient’s perception of pain, since the nature of pulp inflammation can only be reliably determined by morphological studies, which are not carried out in the clinic.
In this regard, the studies of Seltzer S. and Bender I. are interesting, which showed that pulp inflammation is a dynamic process and it does not proceed uniformly from stage to stage, and even using morphological diagnostic methods, it is not always possible to accurately differentiate the acute and chronic course of the inflammatory process, since different forms of inflammation can simultaneously be detected in different parts of the pulp.[4].
Therefore, in the classification of pulpitis, the term "acute" should be used only as a fact of the painful course of pathology, while "chronic" should mean a painless course of pathology. At the same time, pain is a rather subjective factor in the diagnosis of pulpitis, and the reaction to pain and its perception vary from patient to patient and depend on the emotional state of the person.For example, when a doctor examines a patient, the pain caused by acute pulpitis may suddenly disappear (chronic pulpitis), which casts doubt on the diagnosis of “acute pulpitis” made literally a minute before.
Thus, when diagnosing the acute and chronic course of a process, a paradoxical situation often arises when, within a fairly short period of time, two completely different, unfounded diagnoses can be made.
This is why Professor Gofung E. was forced to admit that due to the lack of reliable diagnostic methods, clinicians are forced to mistakenly pay primary attention to the nature of pain, which is a very subjective diagnostic feature [2]. At the same time, the degree of pain does not correlate with pathological changes in the pulp.Indeed, in some cases, destructive processes in the pulp cause painful sensations, and sometimes, on the contrary, do not cause painful sensations.
Based on this, a logical question arises: is it worthwhile at all in clinical conditions to distinguish the main forms of the inflammatory process, if their diagnosis is so problematic, and is it not sufficient to indicate such forms of pulp inflammation only in the anamnesis data of the medical history?
In this regard, the approach to this problem by American scientists deserves attention; they do not use the concepts of acute and chronic inflammatory processes in their classification.At the same time, it is difficult to agree with the American Association of Endodontists (AAE), which, depending on the presence or absence of pain during diagnosis, uses rather inappropriate, in my opinion, terms “symptomatic irreversible pulpitis” and “asymptomatic irreversible pulpitis” [3].Definitely asymptomatic irreversible pulpitis, especially if it occurs in a carious tooth and even occurs without pain, is in all cases without exception a symptomatic disease, since there are no diseases without symptoms.
In addition, the very structure of the construction of some classifications of pulpitis is surprising.For example, in the classification of Walton and Toranbinejad, along with reversible pulpitis, these authors separately distinguish irreversible hyperplastic pulpitis (pulp polyp), as a result of which it is unclear why this classification does not identify other irreversible forms of pulpitis, such as: "pulp fibrosis", "pulp abscess", which are also easily diagnosed by the objective state of the extirpated pulp[5].
However, the greatest controversy arises from the interpretation of the nosology “initial pulpitis” in the WHO classification , since this form includes diseases with different clinical and morphological data: “pulp hyperemia” and “reversible developed pulpitis”, for the treatment of which completely different methods are used (direct and indirect pulp capping)[1].
The WHO classification clearly states that the nosology of “initial pulpitis,” in the treatment of which direct pulp capping is performed, should only include that form of initial pulpitis in which an accidental opening of the pulp cavity occurred due to trauma to an intact tooth or during the treatment of dense, uninfected layers of mantle or circumpulpal dentin.In this case, it is indeed an initial inflammation of the pulp, since the pulp was not infected or inflamed by microorganisms before the opening. If the penetration of microorganisms into the dental pulp can be prevented in time by direct pulp capping with medicated liners, then it may be possible to preserve the pulp.
However, if a perforation of the pulp cavity has occurred as a result of a non-selective method of removing softened infected circumpulpal dentin, then this form of pulpitis is illogical to consider as initial pulpitis in the form of hyperemia, since in this case microbes have already penetrated the pulp due to the lack of protective and adaptive layers of sclerosed and reparative dentin, causing advanced inflammation of the pulp, complicated by injury.
The same can be said when the softened dentin is not completely removed (selective method) and the unopened tooth pulp is separated from the bottom of the prepared cavity only by a thin layer of softened demineralized circumpulpal dentin, the removal of which will lead to the opening of the pulp cavity.Clearly, in this case, microbes have also already penetrated the pulp, causing developed inflammation, and therefore indirect capping of the pulp is carried out to relieve inflammation of the pulp.If it is possible to prevent the complete transformation of caries into pulpitis, then it will be possible to preserve the pulp.
Based on this, a rather paradoxical situation arises when, in the WHO classification of pulpitis, pathology with initial inflammation of the pulp "pulp hyperemia", in which direct capping is used, and pathology with clearly developed inflammation of the pulp "reversible developed pulpitis", in which indirect capping is used, are unreasonably attributed to the same nosology "initial pulpitis"[1].
Moreover, the diagnosis of reversible forms of pulpitis, in the treatment of which biological methods of pulp preservation are used, is still carried out differently in different countries, classifying these nosologies as different diseases (caries or pulpitis).For example, in Russia, indirect pulp capping is performed for caries (deep caries)[2], while the WHO uses this technique in the treatment of pulpitis[1].Even more paradoxical is the position of AAE and ESE, which diagnose even pathologies that spread into the pulp and into the root canal system as “advanced caries” and “extremely deep caries”, in the treatment of which they use biological methods of preserving pulps[3][6].
Doesn't such different diagnostics of the same pathologies violate the generally accepted diagnostic and classification tactics in medicine?
Thus, at present, there is a need for a classification of reversible and irreversible forms of pulpitis, which will eliminate the above-mentioned shortcomings, and which will strictly distinguish between nosologies, in the treatment of which invasive and non-invasive treatment methods are used.
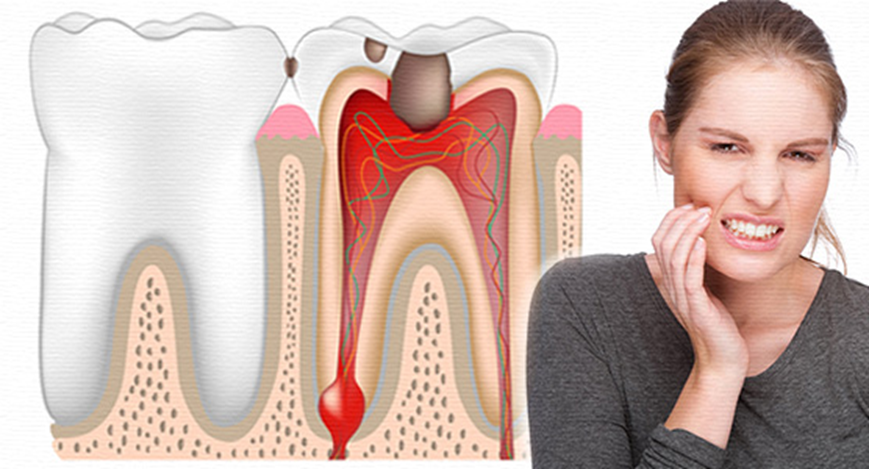
Comparing the majority of currently existing classifications, one can notice that what they have in common is the presence of the nosology “hyperplastic pulpitis” (Fig. 1), the identification of which does not cause any disagreement [5].This is primarily due to the fact that, unlike other nosologies of pulpitis, the diagnosis of this form is quite simple and at the same time reliable, since in this case the emphasis is not on such rather subjective data as the patient's anamnesis and complaints, but on a visual examination of the condition of the inflamed pulp itself, the main diagnostic object.
Fig. 1.Hypertrophic pulpitis.
Unfortunately, this cannot be said about other forms of pulpitis, the diagnosis of which does not pay attention to the objective condition of the extirpated pulp.Unfortunately, dentistry is perhaps the only medical discipline in which, when diagnosing pulpitis that has undergone surgical intervention, objective data from the removed organ (pulp) in relation to which the diagnosis is made is not fully utilized, and, what is most surprising, many clinicians are still not at all bothered by this situation.
This is precisely why not a single textbook on therapeutic dentistry describes the fundamentals of the fundamentals—the objective state of the extirpated pulp, essentially the main object of diagnosis, which is clearly a violation of generally accepted medical rules for making a diagnosis during surgical interventions?
However, paradoxically, an experienced clinician will never make a final clinical diagnosis without taking into account the objective data of the extirpated pulp or what remains of it, as well as without assessing the condition of the pulp cavity and apical foramen.In this case, the main attention is paid to: the integrity of the pulp structure, the presence of hemorrhages, purulent pulp melting, granulations, calcifications, the degree of destruction of root dentin, as well as its adhesion to the pulp, etc.
It is these data that are the main diagnostic features of irreversible forms of pulpitis, and not the sign of pain and its duration, which are quite subjective factors in the diagnosis of pulpitis.
On this basis, I would like to propose a completely new structure for classifying irreversible forms of pulpitis, in which a preliminary diagnosis is made based on medical history, patient complaints and objective examination of the carious tooth cavity, X–ray data, and the final clinical diagnosis is made after surgery as a result of visual examination of the extirpated pulp and the condition of the pulp cavity.
This approach, unlike the current one, does not violate the generally accepted principle of diagnosis during surgical interventions, which states that, based on the patient's complaints and an objective examination of the pathological process, only a preliminary diagnosis is made, and the final diagnosis is made only after surgical intervention!
That is why, to diagnose the objective state of extirpated pulp, I propose to distinguish four visual varieties that are often found in the clinic and are quite easy to diagnose :
1) Pulp - in the form of a dense, elastic, whitish-pink cord, sometimes with areas of hemorrhage.
2) Pulp – grayish or greenish-brown in color, edematous, with areas of purulent and exudative pulp melting, sometimes with a specific odor. The integrity of the pulp may be completely intact, although it is possible to extirpate the pulp in parts.
3) Pulp – in the form of a partial or continuous dense mineralized fibrous cord with a light grayish tint.
4) Pulp – pinkish-gray, slightly edematous, elastic, proliferating from the pulp cavity in the form of granulation tissue.
Often, in some of the listed types of extirpated pulp, denticles and other calcifications are tactilely detected[7]. Moreover, in the absence of anesthesia, the third type of objective state of extirpated pulp is removed relatively painlessly.
The listed pulp types are characteristic of many forms of pulpitis, the diagnosis of which is straightforward. And, most importantly, these pulp types often fully or partially coincide with the histological condition of the pulp. It's surprising how this important fact has remained largely unnoticed.
It's important to note that the first type of extirpated pulp is diagnosed in the early stages of pulp inflammation, when the pulp has undergone functional changes, but its integral (unitary) structure is still preserved. Therefore, it's appropriate to refer to this form of pulpitis as "unitary pulpitis" (Fig. 2).
Fig.2. The first type of objective condition of the extirpated pulp (unitary pulpitis).
An important diagnostic guideline in diagnosing this form of pulpitis is a sign that I called the symptom of “pulp detachment resistance”.This symptom indicates sufficient adhesion of the pulp with the root dentin, as a result of which, when extirpating the pulp, which has not yet undergone destruction, the doctor tactilely feels some resistance and elasticity when tearing the pulp away from the root dentin.During extirpation of destructive forms of pulpitis, such a sensation practically does not arise, which indicates significant destructive disturbances in the structure of the pulp.
Patients with unitary pulpitis complain of a deep carious cavity, food getting stuck, and sharp pain caused by thermal, mechanical, and chemical irritants.A characteristic symptom is the occurrence of spontaneous pain without the influence of irritants, radiating to different parts of the head and intensifying at night.However, with this objective state of the pulp, spontaneous pain may be absent altogether, or only pain from thermal stimuli may be observed. This fact once again demonstrates the subjective nature of pain, which cannot be used as a primary diagnostic guide.
Radiographically, no changes are observed in the tissues surrounding the tooth root. These data only allow a preliminary diagnosis, and a definitive diagnosis is made only after preparation of the carious cavity and extirpation of the pulp, which corresponds to the first type of objective state of the extirpated pulp.In the acute course of this form of pulpitis, it is often necessary to use the extirpation method of treatment, although in the case of a favorable painless course of the process, biological methods of treatment are possible.
The remaining three types of extirpated pulp are found in irreversible destructive forms of pulpitis, in which the pulp has undergone purulent melting (pulp abscess), fibrous transformation (pulp fibrosis) and proliferation (pulp polyp)[1].
Thus, the main diagnostic guideline and criterion for the severity of the pathological process in the pulp is not the nature of the pain or the objective condition of the carious cavity, but the objective condition of the extirpated pulp and root canal itself, especially since pulpitis is not detected radiologically, and the method of electro-dental diagnostics is rather unreliable.It is for this reason that the tactics of constructing a classification is certainly justified, in which the main emphasis is placed on the visual objective state of the extirpated pulp, the main diagnostic object.
Results and discussion
Based on the above, I propose a clinical classification of pulpitis, which distinguishes between reversible and irreversible forms of pulpitis, as well as special forms of pulpitis:
Reversible pulpitis
• Reversible initial pulpitis(initial pulpitis)
• Reversible developed pulpitis
Reversible рartial pulpitis
• Reversible partial pulpitis(reversible coronal pulpitis
• Reversible full pulpitis( reversible root pulpitis)
Irreversible pulpitis
• Unitary pulpitis
• Hyperplastic pulpitis (pulp polyp)
• Purulent pulpitis (pulp abscess)
• Fibrous pulpitis (fibrosis of the pulp)
• Unspecified pulpitis
Irreversible partial pulpitis
Special forms of pulpitis
• Traumatic pulpitis
• Retrograde pulpitis
• Concremental pulpitis
• Residual pulpitis
• Idiopathic pulpitis
At the discretion of clinicians, it is possible to distinguish the category of “normal pulp” in the proposed classification, although, in my opinion, it is more logical to distinguish it in the classification of pulp conditions.You can read more about this in my article “Modernized classification of diseases and conditions of the pulp by Khidirbegishvili” (https://dzen.ru/a/ZF8noiUGsnJ5WXE0).This category in the classification is used to designate pulp that does not have signs or symptoms indicating its pathological changes, since such pulp, although visibly asymptomatic, may be histologically altered as a result of previous trauma or other influences.Normal pulp gives a mild and short-term reaction to cold irritants with mild pain that lasts no more than 1–2 seconds.Clinically, normal pulp does not respond to thermal stimuli (PV Abbott, 2007).
At the same time, it is difficult to agree with the tactics of detecting reversible and irreversible pulpitis in the AAE classification and in other classifications used without identifying numerous forms of this pathology[3].Obviously, such tactics of classifying pulpitis will not reflect the true pathological nature of this common pathology.
It is also important to note that the interpretation of reversible pulpitis in this classification, unlike the WHO classification, does not violate the generally accepted principle of diagnosis during surgical procedures, since direct and indirect pulp capping is performed for completely different nosologies (initial pulpitis and reversible developed pulpitis), which are highlighted separately in the classification, and not classified as "initial pulpitis" (see above ).Of course, this tactic is an obvious advantage of the proposed classification.
As for irreversible forms of pulpitis (pulp abscess, pulp fibrosis and pulp polyp) and special forms of pulpitis (traumatic pulpitis, retrograde pulpitis, calcareous pulpitis, residual pulpitis and idiopathic pulpitis), they are identified in many classifications used today and are easily diagnosed in the clinic[1][7].At the same time, the clinical picture of these pathologies does not differ from those described in many textbooks on therapeutic .
As for special forms of pulpitis, at the discretion of clinicians, it is also advisable to separately identify a combined or combined special form of pulpitis.This is due to the fact that sometimes the inflammatory process in the pulp is accompanied by destructive changes in the alveolar bone.Moreover, these destructive processes can be caused by the direct penetration of infection from the still inflamed, but not necrotized pulp into the bone tissue , or at the same time, the inflammation of the pulp can be accompanied by destructive processes resulting from the penetration of infection into the alveolar bone through a pathological dentogingival pocket.In such a case, a comprehensive diagnosis of pulpitis and alveolar bone destruction should be made.
In addition, some seemingly irreversible special forms of pulpitis in the proposed classification may also be reversible. For example, in the case of concrementous pulpitis, when the denticle is located in the coronal pulp, after its removal, direct root pulp capping can be performed (Fig. 3) [8].
Fig.3. Denticles in the crown of the tooth.
It is also important to note that there is now increasing evidence that infection and inflammation of the pulp, even in a seemingly irreversibly inflamed pulp, can be controlled[7].This is evidenced by experiments with radioactive isotopes of calcium (N. Samr, 1997), which showed that mineralization of the softened infected dentinal bridge occurs not only due to the use of therapeutic pads, but also calcium from the blood[8].
Indeed, over the years of practice, many practitioners have received positive results performing pulpotomy at the request of a patient with irreversible forms of pulpitis.That is why today AAE and ESE have implemented a paradigm shift by offering the possibility of performing a pulpotomy in the treatment of irreversible pulpitis[3][6].On this basis, the nosology that has undergone such treatment can be called “irreversible partial pulpitis” and, at the discretion of clinicians, can remain highlighted in the classification of pulpitis.
Definitely irreversible partial pulpitis differs from reversible partial pulpitis both in its clinical manifestation and in the specifics of the biological treatment of irreversible pulpitis.For example, in the treatment of irreversible partial pulpitis with extensive destructive lesions of the crown pulp, using a direct coating of the root pulp with a therapeutic pad, it is sometimes necessary to remove the inflamed mouth part of the root pulp.
It is also important to note that special attention should be paid to the diagnosis of pulp in a condition where the crown of the tooth pulp is susceptible to necrosis, and the root is simply inflamed or the pulp is inflamed in one of the tooth roots and completely necrotic in the other. This condition was first identified by Professor Grossman Louis, calling it "pulp necrobiosis." Many clinicians refer to this condition as "partial necrosis"[8].When treating such lesions, it is permissible to perform endodontic treatment in one of the canals with biological root treatment in other canals with normal inflammation. Moreover, it is advisable to make a comprehensive diagnosis.
Thus, when treating reversible forms of pulpitis, the following biological methods of pulp treatment should be distinguished:
• Indirect pulp capping
• Direct pulp capping
• Direct partial pulp capping
• Direct root pulp capping
Indirect pulp capping is mainly performed with the selective removal of carious dentin, when, due to the danger of opening the pulp, the doctor leaves some part of the softened circumpulpal dentin on the dentin bridge. When diagnosing such pathology in the case of a positive outcome of treatment, it is advisable to make a diagnosis of "reversible developed pulpitis"and cover the softened demineralized dentin bridge with a therapeutic pad.
Direct pulp capping is performed when the pulp is accidentally exposed due to trauma to an intact tooth or when preparation dense and uninfected layers of mantle and circumpulpal dentin using a non-selective method.This technique should be performed if the exposed defect is up to 3 mm in size and pulp bleeding can be stopped promptly. This condition should be diagnosed as "incipient pulpitis" or "reversible initial pulpitis," and treatment involves covering the exposed pulp with a therapeutic pad.
Direct partial pulp capping is performed when the pulp has already been exposed by the carious process or exposed during the preparation of softened demineralized dentin using a non-selective preparation method and the size of the exposed defect is more than 3 mm.A prerequisite for carrying out this technique is the timely cessation of bleeding and a visually determined limited inflammatory focus without destructive changes in the pulp.This lesion should be conditionally diagnosed as “reversible partial pulpitis” or “reversible coronal pulpitis”, the treatment of which involves partial removal of the coronal pulp with the application of a therapeutic pad to the remaining coronal pulp.
Direct root pulp capping is performed when the pulp has already been exposed by the carious process or exposed during the preparation of softened demineralized dentin using a non-selective preparation method and the size of the exposed defect is more than 3 mm.A mandatory condition for carrying out this technique is the timely cessation of bleeding and visually determined pronounced destructive changes in the pulp.This type of lesion should be conditionally diagnosed as “reversible complete pulpitis” or “reversible root pulpitis”, in the treatment of which the coronal pulp is completely removed, and a therapeutic pad is placed on the root pulp.
Detailed information on selective and non-selective methods of removing carious dentin, the clinical presentation of the nosologies considered, and biological treatment methods can be found in this article of mine (https://dzen.ru/a/ZF5MYlI3ImYriyAT).
Thus, the pulp is completely preserved only with reversible developed pulpitis and initial pulpitis, and in the other proposed nosologies, the pulp is partially or completely removed.In addition, it is important to note that only the diagnosis of initial pulpitis does not cause any particular difficulties due to the cause of its occurrence and the choice of treatment tactics, although it is impossible to predict the outcome of treatment of this nosology.
Special difficulties arise in the diagnosis of reversible developed pulpitis, reversible partial pulpitis and reversible full pulpitis, since it is sometimes difficult to determine the degree of infection and destruction of the crown and root pulp.That is why the diagnosis of reversible forms of pulpitis should always be considered as "preliminary", since it is impossible to be completely sure of the pulp's ability to recover.
Thus, with the progression of the carious process in the dentin and pulp of the tooth, the following completely different nosologies are diagnosed : "dentine caries", "arrested dentine caries", "initial pulpitis", "reversible developed pulpitis","reversible crown pulpitis", "reversible root pulpitis", "irreversible forms of pulpitis" and "special forms of pulpitis".Moreover, before the opening of the pulp cavity and the formation of irreversible forms of pulpitis, only : "dentine caries", " arrested dentine caries" and "reversible developed pulpitis".
Thus, in order to eliminate the confusion regarding the accessories of these nosologies by various dental schools to caries or pulpitis, it is necessary to finally recognize that only two of them (“dentin caries”, “arrested dentin caries”) refer to caries, and the rest to pulpitis.As for the nosologies "dentine caries" and "arrested dentine caries", can read more about these nosologies in my article "Modern clinical classification of Khidirbegishvili's caries"( https://dzen.ru/a/ZF5NT0EW72xkUWOe).
RESULTS AND DISCUSSION
Comparing the proposed classification of pulpitis with the currently used modern classifications proposed by W. J. Walters and D. Hashem, a number of significant differences can be noted.As is well known, Walters proposed a symptomatic system with four different categories of pulpitis: incipient, mild, moderate and severe pulpitis with pulp exposure[9].
Hashem and her colleagues classified pulpitis as[10] :
• mild reversible pulpitis: sensitivity to hot, cold and pain lasting up to 15–20 seconds and spontaneously resolving.
• severe reversible pulpitis: pain increases over more than a few minutes and requires oral analgesics.
• irreversible pulpitis: constant dull throbbing pain, sharp spontaneous pain and tenderness on percussion or pain that increases in the lying position.
Unfortunately, the proposed classifications, in my opinion, are not without significant drawbacks, since, for example, in a clinic it is difficult to differentiate between initial, mild, and moderate pulpitis only based on patient complaints and pain factor.Moreover, this is not a classification of various forms of reversible and irreversible pulpitis, but in fact simply a classification of various categories of pulpitis without identifying the corresponding nosologies of pulpitis.
At the same time, it is necessary to understand that the factor of acute aching spontaneous pain does not always indicate the irreversibility of the lesion, since it does not correlate with the specific histological picture of the tooth pulp.At the same time, the short-term reaction of the pulp to cold and thermal stimuli, which is a sign of reversible pulpitis, does not always reliably indicate the reversibility of the pathological process [7].
Clearly, the pain factor and its duration are quite subjective in pulpitis diagnosis. For example, as mentioned above, during a doctor's examination of a patient, the pain caused by acute pulpitis may suddenly disappear, casting doubt on the diagnosis made just minutes earlier.Тhis is why, when diagnosing reversible forms of pulpitis, the main attention should be paid to the objective state of the dentinal bridge, and not the pain factor.
Thus, attempts to link the nature of pain with the reversibility and irreversibility of the pulp and its condition have not always been justified, since, according to Simon, there is no correlation between the severity of pain and the histological state of the pulp (i.e., the same histological state of the pulp can be painful and painless).
Despite this, Walters, while emphasizing the nature of pain, still attempted in his article to link the pulp categories he proposed with their histological condition[9]. Furthermore, by emphasizing pulp exposure only in severe pulpitis, Walters does not take into account pulp exposure in other proposed forms of pulpitis. At the same time, insufficient attention is paid to initial pulpitis (see above).
At the same time, he unequivocally stated in one of his articles that biological treatment methods are supposedly more reliable than endodontic treatment, which, in his opinion, causes the most complications[9].Unfortunately, in this case, Walters did not take into account that any poor-quality treatment can lead to complications, and high-quality endodontic treatment, unlike high-quality biological treatment, is significantly reliable.
It got to the point that Walters, adhering to the modern tactics of "Endovital", in case of difficulty stopping bleeding during direct partial capping of the root pulp, even advises filling the canal with gutta-percha and siler up to 3-4 mm from the X-ray tip, leaving part of the root pulp alive[9].In this case, an experienced clinician does not take into account that the majority of complications during endodontic treatment under anesthesia are associated with under-sealing of the canal.
It is also noteworthy that the word “irreversible” was removed from all diagnoses in the proposed classification Walters[9]. Although this represents a potentially more relevant diagnostic system, there are currently no studies examining its usefulness for determining the predictability of vital pulp treatment (VPT) procedures.
As for the Hashem classification itself, if a patient needs to be given oral analgesics to relieve pain, then this is no longer severe reversible pulpitis, but, most likely, irreversible pulpitis. In addition, Hashem does not place any emphasis on spontaneous nocturnal pain, which is the most characteristic symptom of irreversible pulpitis[10].At the same time, the proposed time limit of pain up to 20 seconds for determining the reversibility of pulp causes disagreement, since it is unclear whether if the pain continues, for example, 25-30 seconds, then this is no longer mild reversible pulpitis[10]? It is also important to note that pain may be completely absent with both reversible and irreversible pulpitis (this is especially often observed with fibrosis and calcification of the pulp).
Apparently, due to the above-mentioned significant shortcomings, the classifications of Walters and Hashem, unlike their European colleagues, were not accepted for use by more progressive and advanced colleagues from China.
As for the tactics of diagnosing reversible forms of pulpitis in my proposed classification, based on the disadvantages of the Wolters and Hashem classifications discussed above, I propose not to distinguish separate categories of pulpitis (initial, mild, moderate and severe pulpitis with pulp exposure), but rather propose tactics for diagnosing reversible forms of pulpitis: initial pulpitis, reversible advanced pulpitis, reversible partial pulpitis and reversible complete pulpitis.
Briefly, the diagnosis of reversible forms of pulpitis is discussed above in the article, where we are talking about biological methods of treatment.In addition, when diagnosing them, attention should be paid to the following indicators : sensitivity to hot and cold, spontaneously passing within a few seconds, absence of daytime and nighttime strong spontaneous aching pain and pain on percussion,the size of the opening of the pulp cavity and, if it is sufficient, then it is necessary to pay attention to the objective condition of the visible area of the pulp and, necessarily, the intensity of bleeding from the pulp.
The latter factor in the case of exposed pulp is quite important, since it directly affects not only the diagnosis, but also the outcome of treatment. Excessive bleeding after pulp exposure is usually associated with increased inflammation, which reduces the ability to recover in the exposed area [11].If pulpal bleeding cannot be stopped for a long time, this indicates that the pulp is irreversible.If there are no signs of bleeding at all in the affected area, then the pulp tissue is most likely necrotic.It is important to note that moderate bleeding inside the root canal leads to a constant influx of stem cells, and bacteria and their toxins play a key role in the direct stimulation of pulp cells and stem cells[5].
Depending on the type of pulp exposure, the time to stop bleeding varies from 1-3 to 10 minutes . Sometimes bleeding must be stopped by pressing with a sterile cotton ball soaked in a solution of sodium hypochlorite, hydrogen peroxide or iron sulfate [11].
Stopping the bleeding is quite important, since a blood clot can prevent the tight contact of the medicinal pad material with the pulp tissue, which will negatively affect the treatment outcome. healing
It is also important to pay attention to indirect indicators of the choice of biological
treatment: the age and physical condition of the patient, the degree of destruction of the tooth crown for the use of inlays and anchor pins, the possibility of using the tooth to support a bridge prosthesis or to attach a removable denture clamp, etc..The patient's ability to pay is also an important factor.
As for the proposed classification of irreversible forms of pulpitis, their diagnosis does not cause difficulties and it does not violate the principle of diagnosis generally recognized in medicine during surgical interventions.Strangely enough, such diagnostic tactics for irreversible forms of pulpitis are not yet used in any of the classifications that exist today, as a result of which the basic principle of diagnosis during surgical interventions is violated.
Opponents of the proposed diagnostic tactics justify this by the fact that, allegedly, at present, dental pulp is removed only with machine files, and not with pulp extractors, as a result of which it is impossible to objectively assess the condition of the removed pulp.In addition, in some cases, the objective condition of the pulp may not correspond to any of the above-mentioned types of pulp condition, or the diagnosis is complicated due to prolonged exposure to arsenic paste or is completely impossible due to the use of the diathermocoagulation technique.
These arguments are clearly not convincing, since it is inadvisable to remove dental pulp with machine files, especially in wide canals, as this can lead to additional infection of the root dentin, periodontium, and even bone tissue.If the pulp from the narrow canals of the tooth has to be removed using machine files or its condition does not correspond to any of the above-mentioned types, as a result of which it is impossible to assess the objective condition of the pulp, then in this case it is logical to make a diagnosis of "unspecified pulpitis."The proposed tactics will help avoid unfounded diagnoses, since it is better to deliberately make a conditional diagnosis of “unspecified pulpitis” than an unfounded clinical diagnosis.By the way, a similar tactic in case of difficult diagnosis is also used in the WHO classification of pulpitis.
CONCLUSION
The nosologies proposed in the new classification of pulpitis are the main forms of manifestation of pulp pathology, and the proposed tactics for constructing the classification will allow scientifically sound diagnoses of pulpitis and will make it easier for clinicians to choose treatment tactics.In addition, they are quite easily diagnosed in the clinic, which cannot be said about some nosologies used today in various classifications of pulpitis, the diagnosis of which is difficult, and sometimes even impossible.
In conclusion, I invite colleagues to take part in the discussion of the proposed new clinical classification of pulpitis and the possibility of its use in clinical practice. I will gratefully accept and take into account all the amendments and recommendations sent.(otari@inbox.ru).
Conflict of interests. The author declare no conflict of interests
Otari Khiribegishvili graduated from the Russian Medical University in 1978 and is engaged in practical, scientific and pedagogical activities in Georgia in the city of Tbilisi for more than forty years.During this time, he has published more than 100 articles in leading dental journals, and in 2005, the Russian Dental Association published his monograph “Modern Cariesology,” which has been adopted for teaching in Russia and many other countries. Thanks to his achievements in the field of theoretical dentistry, his photo was featured on the cover of the Russian magazine Maestro of Dentistry (No. 1(10)2003). He is the author of classifications of caries, pulp diseases, pulpitis, and periodontitis, which can be used to make informed diagnoses of these major dental diseases!
REFERENCES
1. World Health Organization. Application of the lnternational Classification of Diseases to Dentistry and Stomatology. Third edition, WHO, Geneva, 1995 ; Fifth Ed., WHO, Geneva, 2013. 125 p.
2. Borovsky E. V. Therapeutic dentistry. - M.: "Medical Information Agency", 2003. - 840 p.
3. American Association of Endodontists (2013) Endodontic diagnosis. https://www.aae.org accessed 3rd September 2018.
4.Seltzer S, Bender IB, Ziontz M. The dynamics of pulp inflammation: correlations between diagnostic data and actual histologic findings in the pulp. Oral Surg Oral Med Oral Pathol 1963;16:846-71;969-77.
5.Torabinejad M. Pulp and periradicular pathosis. In: Walton RE, Torabinejad M, eds. Principles and practice of endodontics. 3rd edn. Philadelphia: WB Saunders Co., 2002:34-37.
6. European Society of Endodontology (ESE) developed by:, Duncan, H.F., Galler, K.M., Tomson, P.L., Simon, S., El‐Karim, I., Kundzina, R., Krastl, G., Dammaschke, T., Fransson, H. and Markvart, M., 2019. European Society of Endodontology position statement: Management of deep caries and the exposed pulp. International Endodontic Journal, 52(7), pp.923-934.
7. Cohen, S. , R. C. Burn; Pathways of the pulp, Mosby , St. Louis 1984.- С. 322.
8.Helwig E., Klimek J., Attin T. Therapeutic dentistry. – Lvov: GalDent, 1999.-P. 228, 57.
9.Wolters, W.J. , Duncan, H.F. , Tomson, P.L. , Karim, E.I. , McKenna, G. , Dorri, M. et al. (2017) Minimally invasive endodontics a new diagnostic system for assessing pulpitis and subsequent treatment needs. International Endodontic Journal, 50(9), 825–829. - PubMed
10.Hashem, D. et al. Clinical and radiographic assessment of the efficacy of calcium silicate indirect pulp capping: a randomized controlled clinical trial. J. Dent. Res.94, 562–568 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
11Asgary S., Parhizkar A. Importance of “time” on “haemostasis” in vital pulp therapy. Eur Endod J. 2021;2021(6):128–129. [PMC free article] [PubMed] [Google Scholar]
12. Ricucci D, Candeiro GT, Bugea C, Siqueira JF Jr. Complex Apical Intraradicular Infection and Extraradicular Mineralized Biofilms as the Cause of Wet Canals and Treatment Failure: Report of 2 Cases. J Endod. 2016 Mar;42(3):509-15. doi: 10.1016/j.joen.2015.12.014. Epub 2016 Jan 28. PMID: 26831049.
13. Emara R., Elhennawy K., Schwendicke F. Effects of calcium silicate cements on dental pulp cells: A systematic review. J. Dent. 2018;77:18–36. doi: 10.1016/j.jdent.2018.08.003.
14. Kochmareva A.S., Makeeva I.M., Shelemetieva G.N., Turkina A.Yu. The use of the autofluorescence diagnostics device for controlled сaries excavation. Stomatology for all. 2024; №1(106): 4—8. doi: 10.35556/idr-2024-1(106)4-8.
15. Schwendicke F, Frencken JE, Bjørndal L, Maltz M, Manton DJ, Ricketts D, Van Landuyt K, Banerjee A, Campus G, Doméjean S, Fontana M, Leal S, Lo E, Machiulskiene V, Schulte A, Splieth C, Zandona AF, Innes NP. Managing Carious Lesions: Consensus Recommendations on Carious Tissue Removal. Adv Dent Res. 2016 May;28(2):58-67. doi: 10.1177/0022034516639271. PMID: 27099358.
16.Baelum V, Hintze H, Wenzel A, Danielsen B, Nyvad B. 2012. Implications of caries diagnostic strategies for clinical management decisions. Community Dent Oral Epidemiol. 40(3):257-266.
17.Banerjee A, Kidd EA, Watson TF. 2000. In vitro evaluation of five alternative methods of carious dentine excavation. Caries Res. 34(2):144-150.
18.Bjørndal L, Demant S, Dabelsteen S. 2014. Depth and activity of carious lesions as indicators for the regenerative potential of dental pulp after intervention. J Endod. 40(4 Suppl):76S-81S.
19.De Munck J, Van Meerbeek B, Yoshida Y, Inoue S, Vargas M, Suzuki K, Lambrechts P, Vanherle G. 2003. Four-year water degradation of total-etch adhesives bonded to dentin. J Dent Res. 82(2):136-140.
20 .Ngo HC, Mount G, Mc Intyre J, Tuisuva J, Von Doussa RJ. 2006. Chemical exchange between glass-ionomer restorations and residual carious dentine in permanent molars: An in vivo study. J Dent. 34(8):608-613.