
Khidirbegishvili O.E.
Dentist. Tbilisi, Georgia
Abstract
The difficulty of creating a generally accepted clinical classification of caries that meets all the requirements of clinicians is associated with the imperfection of diagnostic methods, the variety of forms and clinical manifestations of carious pathology, as a result of which it is sometimes difficult to determine the resistant status of carious pathology.It is precisely because of the problems of caries diagnostics that the article proposes a clinical classification of caries that takes into account the positive aspects and shortcomings of the classifications used, including the WHO classification.As a result, the proposed clinical classification, which formulates the principles of constructing a modern classification and examines new nosological forms, allows us to take into account the entire diversity of forms of manifestation of the carious process and is more convenient for use in the clinic.
Keywords : cаries classification system;enamel caries, medium caries, deep caries, progressive dentine caries, initial pulpitis, cement caries.
INTRODUCTION
Dental caries is one of the oldest and most common human diseases. The history of dentistry dates back to 5000 BC, when it was believed that the cause of caries was the "tooth worm". The term "dental caries" first appeared in literature around 1634 and comes from the Latin word "caries", which means decay, destruction of a tooth.
Modern cariesology has reached a sufficient level of development to date to provide clinicians with adequate knowledge in the field of etiology, clinical presentation and treatment of caries. However, strangely enough, there is still no clinical classification of caries that would fully meet the requirements of clinicians.
The clinical classification of caries based on the depth of the lesion (spot stage, superficial caries, medium caries, deep caries) does not adequately reflect the diversity of forms of manifestation of the carious process and does not provide sufficient information about the condition of tissues affected by caries.This classification was proposed in 1948 by I.G. Lukomsky and was intended for the use of cements and amalgams, and not composites, which appeared on the market only in 1962[1].
It is unlikely that I.G. Lukomsky would have proposed such a classification if at that time there were adhesive systems and modern filling materials, the use of which depends not so much on the depth of the lesion, but on the quality of the tooth tissue affected by the carious process, especially since the classic carious process consists of five zones, not one[2].
Moreover, the linear interpretation of such a multifaceted and diverse in its manifestations pathology as caries does not really reflect the essence of the pathological and protective-adaptive processes occurring in this case [2].This is precisely why, when protective and adaptive layers of the carious process (sclerotic and replacement dentin) are formed, medium and deep caries are, in principle, treated in the same way, since there is no need to use protective and therapeutic pads.It turns out that in this case the depth of the lesion is absolutely irrelevant and therefore there is no need to give primary importance to the depth of the carious process[2].
There is no doubt that it is sometimes easier to determine the presence or absence of protective layers of sclerotic and replacement dentin in the prepared cavity than the exact depth of the lesion, especially on the lower jaw incisors.
This is why it is difficult to agree with the ADA CCS system, which divides the radiographic depth of the carious process into difficult to determine lesion sizes (E0 - no lesion, E1 - lesion within the outer half of the enamel, E2 - inner half of the enamel, D1 - outer third of dentin, D2 - middle third of dentin and D3 - inner third of dentin), which clearly complicates diagnosis [3].In this case, it is not taken into account that, for example, the thickness of the enamel varies in different areas of the tooth, so it is not always possible to accurately determine the proposed dimensions of the lesion.In addition, radiographic extent does not always accurately correspond to the stage and depth of the lesion, especially for occlusive lesions, making high-quality diagnostics impossible.
Moreover, it is difficult to agree with clinicians who make the diagnosis of “superficial caries” [2].If we take into account that the average thickness of enamel in different areas of the tooth is from 0.6 to 3 mm, and at the level of the tooth neck it ends completely, then it is surprising how some clinicians manage not only to diagnose superficial caries, but also to fill it without fixing the filling in the mantle dentin (dentin caries).This is why, over the course of many years of practical work, I have never been able to diagnose superficial caries[2].
By the way, the European Endodontic Society (ESE) calls this nosology “moderate caries” or “moderate severity caries”, which has penetrated the enamel but has not yet reached the underlying dentin[4].One can only guess how clinicians who make such virtual diagnoses differentiate such lesions from a pigmented spot, which is characterized by damage to the enamel without penetration into the dentin.
It is also important that the topographic classification takes into account the course of the carious process only in enamel and dentin, as a result of which it does not pay attention to the carious process in cementum, the clinical picture and treatment of which has its own characteristics [2].Based on this, in modern conditions there is a need for a classification of caries that would reflect not only the quality of tissues affected by the carious process, but also take into account the characteristics of the course of the carious process not only in enamel and dentin, but also in cement.
As is known, a similar course of the carious process in various dental tissues is considered in the anatomical classification of the WHO (ICD-10) [5]:
K02 Dental caries
K02.0 Caries limited to enamel
White spot lesion (initial caries)
02.1 Caries extending into dentine
K02.2 Caries of cementum
K02.3 Аrrested dental caries
K02.4 Odontoclasia
Childhood melanodentia. Melanodontoclasia is excluded: internal and external pathological tooth resorption (K03.3)
K02.8 Other specified dental caries
K02.9 Dental caries unspecified
The undoubted advantage of this classification is not only taking into account the characteristics of the clinical course and treatment of the carious process in cementum, but also the exclusion from the clinical manifestations of the carious process in enamel of the nosology “superficial caries”, which, due to diagnostic problems, does not make sense to single out in the classification at all [5].
As for root caries or cement caries, it should be noted that cementum contains less minerals than enamel, and is therefore more vulnerable to the demineralization process than enamel. In addition, it is initiated not by Str. mutans, but by Actinomyces viscus and its transformation occurs without the “white spot” stage[6].At the same time, the roots of teeth have a very thin layer of cement, which contributes to the more rapid progression of the carious process in the root dentin, the structure of which is somewhat different from the coronal dentin (root dentin contains fewer dentinal tubules than coronal dentin) [4].
At the same time, in cement at the early stages of damage, preventive measures can prevent its progression.To do this, according to the recommendation of the German scientist E. Delvig, it is sufficient to remove the demineralized area of cement with an excavator or a spherical burr, and then carry out several applications of fluoride-containing varnish or gel (remineralizing therapy)[8].This is why, in the era of minimally invasive dentistry, at the discretion of clinicians, it is possible to distinguish the nosology of “initial root caries” [2].By the way, in the 1995 WHO classification, this form of cement caries was initially distinguished, but subsequently, for some reason, this tactic was, in my opinion, unreasonably abandoned [5].
In case of significant damage to cement and root dentin, surgical and restorative treatment is carried out, which also has its own characteristics associated with the problematic bonding of adhesive systems and composites with tooth cement.In addition, when filling root caries that extends to the crown of the tooth, it is necessary to simultaneously create conditions for adhesion to the enamel, cement, coronal and root dentin, which is extremely difficult [2]. Based on the above, the treatment of such root lesions is sometimes problematic.
A significant drawback in the WHO classification is also the inclusion of only a white spot as enamel caries, while a pigmented spot, which is characterized by the integrity of the enamel-dentin border, is singled out separately as a arrested caries.At the same time, it is difficult to agree with the lack of a separate allocation in the classification of various forms of arrested caries in dentin and cement, the treatment of which has its own characteristics[5].
Scientists Bushan M. G. and Kodola N.A. have unequivocally proved that the development of the carious process can stop at any stage of development due to increased hypermineralization of tooth tissues[7].Is it really true that in such a complex and multifaceted pathological process as caries, nature has not provided a mechanism of protection not only against the spread of the carious process from enamel to dentin (pigmented spot), but also from dentin to pulp[2]?
This is precisely why the allocation in the WHO classification of only one form of arrested caries (pigmented spot) [5] is clearly insufficient, especially since sometimes, as a result of enhanced remineralization, not only all tooth tissues are mineralized, but even in deep cavities the pulp manages to form a significant layer of replacement dentin, which differs significantly in its mineralization from the replacement dentin formed in a normal carious lesion (Fig. 1).
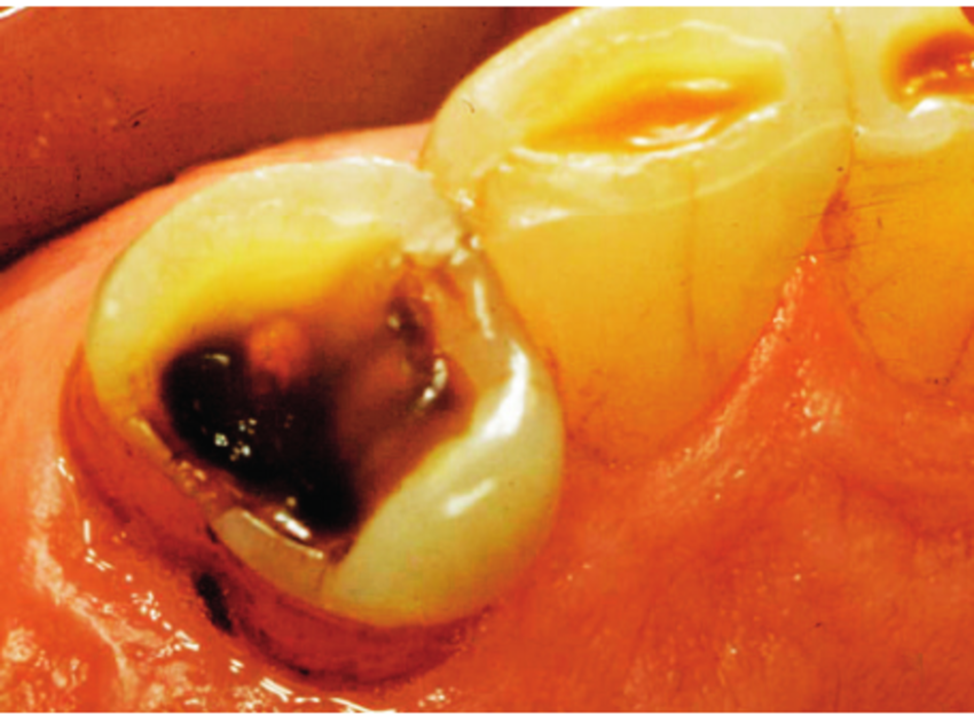
Fig.1. Аarrested dentin caries in a deep carious cavity of a premolar.
Undoubtedly, with sufficient resistance of the body and other favorable conditions, the carious process in enamel, dentin and cementum can proceed more slowly or even stop completely, which is why it is also called “stationary caries” [8].In this form of caries, due to the high mineralization of enamel and dentin, even in a deep carious cavity, pain is not observed and, what is especially important, the development of the carious process stops.
More often, this course of caries is noted on the occlusal surfaces of teeth, which are subjected to abrasion during chewing, as a result of which the carious defect, which has undergone a similar effect, is completely mineralized (Fig. 2).In the process of increased hypermineralization, the exposed surface of dentin, devoid of enamel, scleroses and becomes vitreous[2].
Fig.2.Аrrested dentine caries on the erased chewing surface of the molar.
Any form of dentine caries can turn into stationary caries, which is most often the outcome of a chronic course, although cases of a direct transition to this form of an acute course of the carious process have been described.The initial and subsequent stages, depending on the depth of the stationary carious process, are characterized by the appearance of intense brown, black-brown dentin coloration in the affected area[8].In this form of caries, a peculiar mineralized "scar" can be found on the hard tissues of the tooth, indicating a carious lesion in the past. Sometimes tooth tissues, due to increased remineralization, become vitreous, as a result of which this form of caries is also called "sclerosed caries"[8].
Thus, in the clinical classification of caries, it is necessary to separately distinguish arrested caries not only of enamel (pigmented spot), but also of dentin and cementum, for the treatment of which various treatment methods are used.
In this regard, it is difficult to agree with the ADA CCS system, which classifies any clearly visible carious lesion on any surface of the tooth as effectively “progressive”[3].That is why a significant addition to the principle of allocation (ADA CCS) of four groups of caries (healthy, initial, moderate and advanced) should be an addition to this system of the group "arrested caries", the importance of a separate allocation of which is discussed above[2].In addition, it is difficult to agree with the use of the concept of "healthy caries", since any pathology is not healthy.
The allocation in the WHO classification of only one form of dentin caries and one form of root caries also raises disagreement[5]..Can the coating of pulp with protective pads, sandwich technique, layered restoration technique and Bertolucci technique be carried out with the same form of dentine caries and root caries [2]? At the same time, various forms of dentine caries are characterized by various types of carious cavities with a diverse combination of carious process zones, as a result of which the clinic and treatment of these lesions have their own characteristics (see below).
In this regard, minor carious lesions in the mantle dentin with progressive lesions in the circumpulpal dentin can hardly be considered identical.Based on this, it is advisable to supplement dentine caries and root caries in the classification with qualitative characteristics of the dental tissues involved in the carious process, highlighting ordinary lesions and arrested lesions[2].
It is also difficult to agree with the allocation of nosology in the WHO classification under the code K 02.9. "Dental caries, unspecified", which is indicated in the case of a carious process in depulpated teeth[5].Moreover, the very reason for the allocation of this nosology is surprising, which is dictated by the fact that in this case it is allegedly impossible to make the usual diagnosis of "dentine caries"
, due to the fact that the currently accepted clinical indicators (response to probing, chemical and temperature stimuli) will be negative due to the absence of pulp.
Are carious lesions with living pulp not diagnosed in the clinic when the above clinical indicators are completely absent? For example, with increased mineralization of enamel and dentin (arrested caries), such signs are completely absent[2].
The same can be said about the nosology under the code K 02.8. “Other specified dental caries”, which is put in the case of secondary and recurrent caries[5].It is unclear what is the point of such a diagnostic tactic, if such carious lesions as types of caries are usually separately diagnosed as "secondary caries" and "recurrent caries".In addition, these lesions can occur in depulpated teeth after filling.
It is also important to note that Professor P.A. Leus in his article “Improving dental caries classifications and their importance in the practice of a dentist” writes that in practice, WHO classification definitions with codes K02.4, K02.8, K02.9 are not actually used [9].
Today, many indices have been developed to assess caries, but none of them can be considered ideal, not even the International Dental Caries Assessment System (ICDAS). Unfortunately, the American Dental Association (ADA) classification of caries [3] is not without significant shortcomings (these shortcomings will be the subject of a separate article of mine).
This statement was also acknowledged by the editor-in-chief of the JADA magazine, Tim Wright, after reading my article.However, his statement regarding my proposed modification of the caries classification ADA is interesting. He stated unequivocally: "Of course, the classification is not without drawbacks, but American doctors are used to it and therefore it makes no sense to modernize it."There is nothing to say, the "wise" and "philosophical" reason for the refusal!
MATERIALS AND METHODS
Based on the above, I propose a clinical classification of caries, which takes into account all the above disadvantages of the classifications considered :
Dental caries
Enamel caries
• The stage of the "white spot" (initial clinical manifestation of dental caries )
• The stage of "pigmented spot" (arrested enamel caries)
Caries of crown dentin
• Dentin caries
• Arrested dentin caries
Caries of cementum and root dentin
• Root caries
• Arrested root caries
A strictly individual designation in the classification of affected dental tissues is, I believe, more informative, although at the discretion of clinicians it will be possible to use the usual less informative designations: enamel caries, dentin caries and root caries.
In addition, а white spot should be considered the initial clinical manifestation of caries, and not the initial caries as in the WHO classification, which should be considered as a result of numerous externally unrecorded changes in the enamel that occur during the process of its infection with bacteria.You must admit that these are completely different concepts.
As for the pigmented spot, in the proposed classification it is not distinguished separately as in the WHO classification, but is classified as enamel caries and is considered to be arrested enamel caries.In the case of dentin progression and damage, it transforms into dentin caries[2].
Fig.3.Pigmented spot .
This form of enamel caries is characterized by light brown, dark brown and black spots, the removal of which does not disrupt the enamel-dentine junction (Fig.3).There are no painful sensations, although sometimes there may be slight pain on cold and hot.Patients mostly complain of a cosmetic defect due to the appearance of dark spots.Moreover, the carious process due to mineralization may not progress for a long time.That is why this form of pigmented spot is considered to be arrested enamel caries[2].
Moreover, Professor Pakhomov believed that only dark brown and black spots are characterized by damage to the enamel-dentine border, while light brown ones are without damage to the enamel-dentine border.However, Professor Borovsky convincingly proved that there are also dark brown and black spots without damage to the enamel-dentin border, since when dentin is damaged, “dentin caries” is already diagnosed[10].
Indeed, a pigmented spot is a spot because it is not characterized by damage to the enamel-dentin border and that is why it is actually a transitional form between enamel and dentin caries!
When treating a pigmented spot, it is enough to remove pigmentation on smooth surfaces and carry out remineralizing therapy. If fissures are affected, their invasive sealing can be carried out, and if the enamel-dentin junction is slightly affected, then extended fissure sealing is acceptable[2].It should be noted that non-invasive fissure sealing is a purely preventive procedure and is performed on teeth not affected by caries.
A separate article will be devoted to the clinical manifestations and treatment of the proposed forms of caries in more detail. However, I would like to separately consider the pathologies related to coronal dentin caries, which differ in diagnostic features and cause the most controversy.
Dentin caries is diagnosed when the protective-adaptive layers of sclerotic and reparative dentin have not formed, and after using a non-selective preparation method, the roof of the pulp cavity consists of a dense but non-mineralized layer of mantle or circumpulpal dentin.In this case, if the dentine bridge is quite dense and not thin, then there is no need to use protective and therapeutic pads during filling, but it is enough to cover the treated cavity with an adhesive system and apply the appropriate seal[2].
If the dentinal bridge is dense but relatively thin, which is usually observed when the circumpulpal dentin is affected, then only protective pads should be used to prevent the traumatic effects of polymerization shrinkage of adhesive systems and filling materials on the tooth pulp.It is precisely because of the different treatment of such pathologies that, at the discretion of clinicians, it is possible to distinguish between caries of the mantle dentin and caries of the circumpulpal dentin.I think it is less informative to use the concepts of "medium" and "deep" in this case (see above).
Arrested dentin caries differs from normal dentin caries by the intensive formation of protective-adaptive layers of sclerotic and reparative dentin, as a result of which there is no pain from cold and hot, and in a deep carious cavity there is no need at all to use protective and therapeutic pads.Moreover, mineralization can be so intense that not only the dentinal bridge of circumpulpal dentin is mineralized, but also the mantle dentin on the walls of the cavity[8].At the same time, sometimes due to strong mineralization, an intense brown, black-brown coloration of the tooth tissue appears (Fig. 1).Sometimes, only the dentinal bridge is subject to intensive mineralization.
It is important that the fixation of composite materials in this form of dentin caries is extremely difficult, since the use of adhesive systems, due to the high mineralization of the affected tooth tissues, is ineffective, unlike conventional forms of dentin caries.Therefore, it is preferable to use glass ionomer cements here, which form a chemical bond with the tooth tissue, or to use the sandwich technique, and sometimes it is more appropriate to cover such teeth with appropriate orthopedic crowns[2].
Particular difficulties with filling arise in prepared cavities in which all tooth tissues have been subjected to intense mineralization and black-brown coloration.Based on this, at the discretion of clinicians, it is possible to distinguish two forms of arrested dentin caries: “partial arrested dentin caries” and “intensive arrested dentin caries” (other names for these nosologies are also possible).
However, the protective and adaptive layers of sclerosed and reparative dentin may not form at all, and as a result of the use of a selective method of removing carious dentin, the dental pulp is separated from the bottom of the prepared cavity by a thin layer of softened demineralized infected circumpulpal dentin.Removal of this softened dentin will definitely lead to the opening of the pulp, since there is no dense demineralized circumpulpal dentin left under this layer[2].
An objective examination of this nosology reveals softened dentin in the carious cavity from gray-yellow to black, affecting the entire thickness of the circumpulpal dentin (Fig. 4)Preparation and probing of this carious cavity is extremely painful. Patients complain of a cosmetic defect, food getting stuck, pain from cold and hot, which disappears immediately after their elimination, although the pain may be longer lasting, and sometimes be absent altogether.Radiologically, no changes are observed in the tissues surrounding the tooth root. The listed data allow only a preliminary diagnosis to be made, and the final diagnosis is made only after preparation of the carious cavity [2].
Fig.4. Objective picture of a carious cavity with softened demineralized circumpulpal dentin.
As a result of removing decayed carious tissues using a selective method, we obtain a prepared cavity within the circumpulpal dentin. The walls of this cavity are dense, and the dentin bridge in the area of the pulp horns consists of a thin layer of demineralized softened dentin.When probing, pain is noted along the walls and bottom of the carious cavity, especially at the points closest to the pulp of the tooth.Moreover, probing the bottom of the prepared cavity and partial removal of demineralized softened dentin from the bottom of the cavity must be carried out very carefully, since at the projection points of the pulp horns the arch of the tooth cavity can be thin, so it can easily be pierced with a probe, opening the pulp of the tooth [2].It is this data that allows us to make a final diagnosis[2].
Oddly enough, no textbook other than mine, Modern Cariesology, examines in detail the objective conditions of the prepared cavities in the diagnosis of carious lesions, as a result of which the diagnosis of caries and other pathologies is often mistakenly made based on patient complaints and the objective condition of the carious cavity that has not been prepared (Fig.5).Clearly, such a diagnostic tactic violates the generally accepted principle of diagnosis during surgical interventions[2].
Fig.5.The difference in the assessment of the condition of dental tissues in carious and prepared cavities.
Paradoxically, it is precisely this nosology that causes the most disagreement and debate, since the question of which disease (caries or pulpitis) these pathologies belong to, the treatment of which involves indirect pulp capping with therapeutic and protective pads, has not yet been definitively resolved.For example, the Dental Association of Russia (StAR) considers such pathologies to be deep caries[10].The American Association of Endodontists (AAE) and the European Endodontic Society (ESE) diagnose similar pathologies, even with opened pulp, as: "advanced caries", "extremely deep caries", "extremely deep caries"[3][4].And only the WHO classifies such lesions, for the treatment of which indirect capping is used, as pulpitis[5].
Doesn't such different diagnostics of the same pathologies violate the generally accepted diagnostic and classification tactics in medicine?
It is definitely difficult to agree with the tactics of StAR, AAE, and ESE, who consider such a pathology, in which the pathological process has already penetrated the pulp, causing chronic inflammation, to be caries [8].Based on many years of practical activity, in my opinion, this nosology should definitely be considered pulpitis, since in this case, due to uneducated protective and adaptive layers, the pulp is already infected and susceptible to chronic inflammation.
At the same time, it is not difficult to imagine the degree of such chronic inflammation, given that inflammatory changes in the pulp occur already during the maturation of plaque in the tooth enamel.At the same time, in this case, not only bacterial toxins, enzymes, and antigens penetrated the pulp, which usually cause pulp hyperemia, but also the bacteria themselves, causing advanced inflammation of the pulp (Trowbridge, 1972).
Definitely, as soon as the pathological process has completely spread into the pulp, causing stress and infection of the dentin-pulp complex, such a pathology should already be diagnosed as "pulpitis", and not "caries".As a result of the deposition of reparative dentin on the walls of the pulp cavity, the pulp volume decreases, the proportion of collagen increases and the cellular composition decreases, which leads to a qualitative decrease in its functions. This condition is called "pulp atrophy"[7].In addition, it is necessary to finally understand that the pulp, after a successful biological treatment method, never returns to the state in which it was during a purely carious lesion[2].
That is why the method of treating such pathology is called "biological treatment of pulpitis", and not caries.After all, for example, pulp pathology that has penetrated into the periapical tissues is already considered periodontitis, not pulpitis. You can read more about the developed periodontal pathology in my article “Clinical classification of inflammatory diseases and conditions of periapical tissues of the tooth according to Khidirbegishvili” (https://dzen.ru/a/ZF8b-kEW72xkS_ZA).
At the same time, when diagnosing such a pathology, a long-term preliminary diagnosis is made (the word “long-term” indicates the duration of determining the treatment result), and then a final diagnosis is made [2].In this case, based on the above, it is advisable to classify this nosology as pulpitis and call it "reversible developed pulpitis"(Fig. 4). This diagnostic tactic is due to the fact that reversible developed pulpitis is a rather unpredictable pathology, since it is difficult to predict the preservation of the pulp in the event of successful indirect capping of the pulp.This is also due to the fact that in this case morphological examination is not carried out, it is impossible to use objective pulp data for diagnosis, and the patient's complaints and the nature of pain are quite subjective diagnostic parameters[2].
That is why in this case it is more logical to make a long-term preliminary diagnosis of "reversible developed pulpitis".If after indirect capping of the pulp and applying a temporary filling for some time (several weeks) there is no exacerbation of the process and it is possible to prevent the complete transformation of caries into developed pulpitis, then only then will the preliminary diagnosis of "reversible developed pulpitis" become final. This is evidenced by the term "reversible" in the name of nosology, which in this case does not mean a natural suspension of the further progression of the carious process into pulpitis due to the body's defenses, but an artificial one using therapeutic pads[10].
In case of successful application of indirect developed of the pulp with therapeutic pads, sclerosed and reparative dentin is deposited on the inflamed pulp, which prevents further infection of the pulp and contributes to further stabilization of the developed inflammatory process in the pulp [9].That is why the nosology "reversible developed pulpitis", along with the nosology "initial pulpitis", in the classification of pulpitis proposed by me (https://dzen.ru/a/ZF5UQ0ej8SbfgCyY) I attributed it to reversible forms of pulpitis.
Unfortunately, the success of treating such a pathology is not always positive, therefore it causes distrust among some clinicians. On this basis, clinicians V.S. Ivanov and L. I. Urbanovich quite reasonably argued that the biological method is discredited not because it is not possible to keep the pulp viable, but because it is impossible to accurately identify the degree and stage of pulp inflammation[7].Attempts to link the nature of pain with the condition of the pulp were unsuccessful, since there is no correlation between the severity of pain and the degree of damage to the pulp (Simon et al. 2013).Based on this, the emphasis should be placed on the possibility of preventing the progressive complete transformation of caries into advanced irreversible pulpitis.
Based on all of the above, reversible developed pulpitis should actually be considered a transitional form between caries and pulpitis, in the treatment of which it is not always possible to stop the further progression of the inflammatory process in the pulp.This approach is also justified by the fact that it becomes possible to justify the legal responsibility of a doctor in the treatment of such a neglected and unpredictable pathology, since by fixing such a diagnosis and warning the patient in advance about possible complications, the doctor, in case of an exacerbation of the process, relieves himself of legal responsibility., if adequate treatment has been performed[2].
It should also be noted, that the use of a selective method of removing demineralized softened circumpulpal dentin in the treatment of reversibly developed pulpitis causes a fierce confrontation between AAE and ESE [3][4].While American clinicians are opposed to this technique, Europeans are strongly in favor of using this technique because of the alleged reduction in the likelihood of pulp exposure.According to the AAE position, complete removal of softened infected dentin increases the chance of successful treatment of such lesions[3].From the perspective of ESE, the preservation of pulp affects the viability of the tooth.,by making it more resistant to destruction, it retains the ability to repair tissues, preventing various complications, etc.[4].
Based on many years of practice, I would like to note that when treating such lesions and choosing a treatment method, first of all, attention should be paid to the patient's age, state of health, the presence of chronic odontogenic intoxication, pronounced periodontitis, the possibility of covering such teeth with orthopedic structures, the patient's ability to pay, etc. It is these factors that sometimes dictate the possibility of using selective and non-selective removal of demineralized dentin, non-opening of the pulp cavity and the choice of treatment tactics, rather than the strict requirements of using these AAE and ESE techniques[3][4].You can read more about this in my article "Selective and non-selective dentin removal and classification of biological methods of pulp treatment" (https://dzen.ru/a/ZF5FY5KsTRJ16Qjh ).
Thus, as the carious process progresses in the dentine and in the tooth pulp with an unopened tooth cavity and the formation of irreversible forms of pulpitis, three completely different nosologies are diagnosed: "dentine caries", "suspended dentine caries" and "reversible developed pulpitis".Therefore, in order to eliminate the complete confusion regarding the interpretation and attribution of these nosologies by various dental schools as caries or pulpitis , It is necessary to finally recognize that only two of them ("dentine caries" and "suspended dentine caries") refer to caries, and "reversible developed pulpitis" refers to pulpitis.
As for cement caries, it occurs mainly in patients over 60 years of age, and the tactics of diagnosis and treatment of carious lesions of root dentin are similar to those of crown dentin.Its occurrence is associated with poor oral hygiene in old age, the presence of areas of exposure of the root surface in periodontitis, decreased saliva secretion, taking medications, etc. Cement caries develops especially intensively in people who have undergone radiation therapy in the head and neck area[6].
RESULTS AND DISCUSSION
Since caries is characterized by a variety of forms of manifestation, it is not enough to diagnose caries using only one clinical classification.Based on this, the multi-system classification of caries is fully justified. : by localization, by the nature and dynamics of the course, by the intensity of the lesion, by the sequence of occurrence of the process, the allocation of special forms of caries, etc..It is also important to consider infant caries, childhood caries, and adolescent caries separately.
Moreover, not all of these clinical manifestations need to be diagnosed in the clinic, since some of them have purely scientific significance. For example, there is no strict need to distinguish acute and chronic caries in the clinic during diagnostics, since caries is, in principle, a chronic pathology [10].
In this regard, it is necessary to agree with Professor E. V. Borovsky, who argued that such a division in the clinic is invalid, since even with an intensive carious process, at least 3-6 months pass from the moment of demineralization until the moment of formation of a carious cavity, which does not fit into the framework of the development of an acute process accepted in medicine [10].
An exception is a rare and special form of caries with partial or complete damage to the salivary glands (extremely acute caries), which occurs within 2-3 weeks, as well as a clinical variant of acute caries with multiple lesions of the teeth, florid caries (caries florida). These forms of caries are clearly characterized by an acute course [2].
It is also important to note that a group from the University of Illinois Faculty of Engineering successfully sequenced the complete genomes of three strains of Streptococcus sobrinus bacteria, as a result of which they concluded that they produce acid more and faster than Streptococcus mutans, which leads to the most severe clinical results, especially in children.It was also found that with the simultaneous action of these two types of bacteria, teeth can break down so quickly that it seems that there is some kind of unknown relationship between them, due to which they act more strongly in combination than alone[11].
It is also important to note that as a result of excessive fluoridation of the enamel during preventive measures, the carious process in the dentin often occurs with the integrity of the enamel.A similar form of dentine caries can only be detected by X-ray examination, where such hidden cavities are defined as areas of lumen in the dentine (hidden dentine caries)[2]. It is with this pathology that patients often complain of increased sensitivity in their teeth without detecting carious lesions. This form of caries, along with acute caries, flowering caries, etc., I think it is advisable to classify it as atypical or special forms of caries[2].
At the same time, when making a diagnosis based on the proposed clinical classification, for a more accurate and detailed diagnosis, in my opinion, it is desirable to use a comprehensive diagnosis of caries, which will also display various characteristics of the carious process that directly affect the choice of treatment tactics [2].
First of all, this refers to the localization of the carious process on the tooth surface (fissure, contact, cervical, circular caries), which sometimes directly affects treatment tactics[10].As is known, due to the complex configuration of the tooth crown with different directions of enamel prisms, the spread of caries and its treatment tactics on different surfaces of the tooth have a number of features.In this regard, we must agree with our colleagues from the ADA, who, due to the problems that have arisen with the use of Black's classification when using modern filling materials, are trying to reconsider its use in our time[3].My article "Paradoxes of modern dental Science" is devoted to this topic (https://dzen.ru/a/ZF5OQ1I3ImYrjw1g), in which I propose a new classification of the localization of carious lesions.
It is also important to take into account the primary and secondary occurrence of the carious process in the clinic.Primary caries is the occurrence of a process in an intact tooth.The occurrence of a carious process in a tooth already affected by caries should be considered secondary and recurrent caries.Unfortunately, the interpretation of secondary and recurrent caries varies in different dental schools and is not always scientifically justified[2].
That is why I would like to offer my own interpretation of these forms of caries.Secondary caries should be considered the occurrence of a carious process in a tooth already affected by caries, as well as outside the boundaries of a previously placed filling.Recurrent caries should be considered the resumption of the carious process at the boundaries of a previously placed filling as a result of poor-quality preparation of the carious cavity, polymerization shrinkage of the filling material, as well as other errors made during cavity filling[2].
However, it is difficult to agree with Professor Borovsky's interpretation of recurrent caries, which focuses on the occurrence of lesions on the border of the filling and under the filling, since such lesions can be combined[10].You can read more about this in my monograph "Modern Cariesology", which is accepted for teaching in Russia and in many post-Soviet countries .
Based on the above, a comprehensive diagnosis of caries, for example, may look like this:
Secondary fissure caries of dentin of tooth 14
Primary arrested caries of the root of tooth 15
A wide variety of combinations of a comprehensive diagnosis of caries are possible, so a separate article will be devoted to this topic.
This tactic of making a comprehensive diagnosis of caries allows you to take into account the variety of forms of the carious process.At the same time, it is more informative, and it also makes it easier to describe the objective picture of the carious process in the medical history.In my opinion, only such a diagnostic tactic will allow a high-quality diagnosis of the carious process.
CONCLUSION
The proposed nosologies in the new clinical classification of caries are the main forms of manifestation of the carious process in tooth tissues, which are easily diagnosed in the clinic.When using them, there are no problems with diagnosis, which cannot be said about some nosologies in the applied classifications of caries, the diagnosis of which is difficult and sometimes impossible.
In conclusion, I would like to know the opinion of colleagues about the proposed classification and the possibility of its use in clinical practice. Gratefully accept and take into account all the amendments and recommendations sent.
The author declares no conflict of interests / The authors declare no conflict of interests
Otari Eduardovich Khidirbegishvili is a graduate of the SSMI in 1978, who has been engaged in practical, scientific and pedagogical activities in the city of Tbilisi for more than forty years. During this time, more than 100 articles have been published in leading dental journals, and in 2005 the Dental Association of Russia published a monograph "Modern Cariesology", which is accepted for teaching in Russia and in many countries. Due to developments in the field of theoretical dentistry, the photo is placed on the cover of the Russian magazine "Maestro of Dentistry" (№ 1(10)2003).He is the author of classifications of caries, pulp diseases, pulpitis and periodontitis, which can be used to make reasonable diagnoses of these major dental diseases!
REFERENCES
1.Lukomsky I. G. Therapeutic dentistry: Textbook. – M., 1955 – 487 p.
2.Khidirbegishvili O. E. Modern cariesology. – Moscow:Medical Book, 2006 - p. 134.6.
3.Young DA, Nový BB, Zeller GG, Hale R, Hart TC, Truelove EL., American Dental Association Council on Scientific Affairs. American Dental Association Council on Scientific Affairs. The American Dental Association Caries Classification System for clinical practice: a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2015 Feb;146(2):79-86.
4. Duncan H F, Galler K M, Tomson P L et al. European Society of Endodontology position statement: Management of deep caries and the exposed pulp. Int Endod J 2019; 52: 923-934.
5. World Health Organization. Application of the lnternational Classification of Diseases to Dentistry and Stomatology. Third edition, WHO, Geneva, 1995 ; Fifth Ed., WHO, Geneva, 2013. 125 p.
6. Banting, dW. The Diagnosis of Root Caries. Presentation to the niH Consensus development Conference on diagnosis and Management of dental Caries throughout Life. March 2001.
7. Bushan M.G., Kodola N.A. Dental caries. State Publishing House – 1975.-P. 114.
8. Barber D, Massler M. Permeability of active and arrested carious lesions to dyes and radioactive isotopes. J Dent Child 1964;31:26- 33.
9. Leus P.A. Classifications of human dental caries: from G.Black to ICDAS // Dental journal. – 2015. – Vol.16, No.1. – P.6–15. /.
10. Borovsky E. V. Therapeutic dentistry. - M.: "Medical Information Agency", 2003. - 840 p.
11. Sánchez-Acedo M, Montiel-Company J-M, Dasí-Fernández F, Almerich-Silla J-M. 2013. Streptococcus mutans and Streptococcus sobrinus detection by polymerase chain reaction and their relation to dental caries in 12 and 15 year-old schoolchildren in Valencia (Spain). Med Oral Patol Oral Cir Bucal 18:e839–e845.
12. Dr. Neromini Fagu. Dental Health-Active Caries vs. Arrested Caries. kaieteurnewsonline.com/2017/03/12/dental-health-activecaries-vs-arrested-caries.
13. Greene Vardiman Black [Online Green]. 2009 [cited 2009 June 2];available from: http://en.wikipedia.org/wiki/Greene_Vardiman_Blac..
14.Ngo HC, Mount G, Tuisova J, Von Doussa RJ. 2006. Chemical exchange between glass-ionomer restorations and residual carious dentine in permanent molars: An in vivo study. J Dent. 34(8):608-613.
15.Paddick JS, Brailsford SR, Kidd EA, Beighton D. 2005. Phenotypic and genotypic selection of microbiota surviving under dental restorations. Appl Environ Microbiol. 71(5):2467-2472.
16.Orhan AI, Oz FT, Orhan K. 2010. Pulp exposure occurrence and outcomes after 1- or 2-visit indirect pulp therapy vs complete caries removal in primary and permanent molars. Pediatr Dent. 32(4):347-355.
17.Monson MA, Banerjee A, Watson TF, Wade WG. 2004. Molecular analysis of the microflora associated with dental caries. J Clin Microbiol. 42(7):3023-3029.