
Khidirbegishvili O.E. Dentist. Tbilisi, Georgia
Abstract
For many years, it has not been possible to definitively resolve the issue of a selective and non-selective method for removing softened dentin, therefore, the article presents data on the application of these techniques in specific clinical cases.The advantages and disadvantages of the applied techniques are described , new nosological forms are proposed , and principles and rules for the treatment of these nosologies by biological treatment methods are formulated.In addition, the article presents the concept– to which disease (caries or pulpitis) should various pathologies be attributed, in the treatment of which biological treatment methods are used.It is the diagnostic and treatment methods proposed in the article that allow for the establishment of sound diagnoses and contribute to the rational selection of an appropriate treatment method.
Keywords: initial pulpitis, reversible pulpitis, irreversible pulpitis, traumatic pulpitis, pulp hyperemia,arrested carious pulpitis, non-selective dentin caries, pulp atrophy.
For citation
Khidirbegishvili O.E.. Selective and Non-Selective Dentin Removal and Classification of Biological Pulp Treatment Methods (review)
INTRODUCTION
One of the priorities of clinical dentistry is the introduction of minimally invasive biological methods of pulp treatment. That is why, in 2015, at the International Conference on Caries Collaboration in Leuven, proposals were put forward that preserving pulp vitality should be considered a priority in the treatment of certain carious lesions.However, the question of which method of removing carious dentin (selective or non-selective) is preferable to use in the biological treatment of inflamed pulp has not yet been finally resolved. In addition, it is still unclear to which disease (caries or pulpitis) various pathologies with unopened and opened pulp belong, for the treatment of which biological methods of pulp preservation are used.
For example, in Russia, such pathologies are strictly differentiated into deep caries and pulpitis[1]. The American Association of Endodontists (AAE) [2] and the European Endodontic Society (ESE) [3] similar pathologies spreading to the pulp and even to the root canal system diagnosed as caries (аdvanced dental caries, ultra-deep caries). Despite this, WHO, on the contrary, classifies all nosologies for the treatment of which biological methods of pulp treatment are used as pulpites[4].
Clearly, such different diagnostics of such pathologies violates generally accepted diagnostic standards in medicine.
At the same time, it is difficult to agree when, in the WHO classification, initial pulpitis includes diseases that differ in clinical and morphological data, for the treatment of which completely different methods are used (direct and indirect pulp capping)[4].
Unambiguously, the nosology of "initial pulpitis", in the treatment of which direct pulp capping is performed, in the WHO classification should include only that form of initial pulpitis in which an accidental opening of the pulp occurred during trauma to an intact tooth or during the preparation of dense and uninfected layers of dentin in the treatment of caries. In this case, we are actually talking about initial inflammation of the pulp (hyperemia), since immediately before the opening, microorganisms had not yet penetrated the pulp and it was not infected and inflamed(Fig.1).
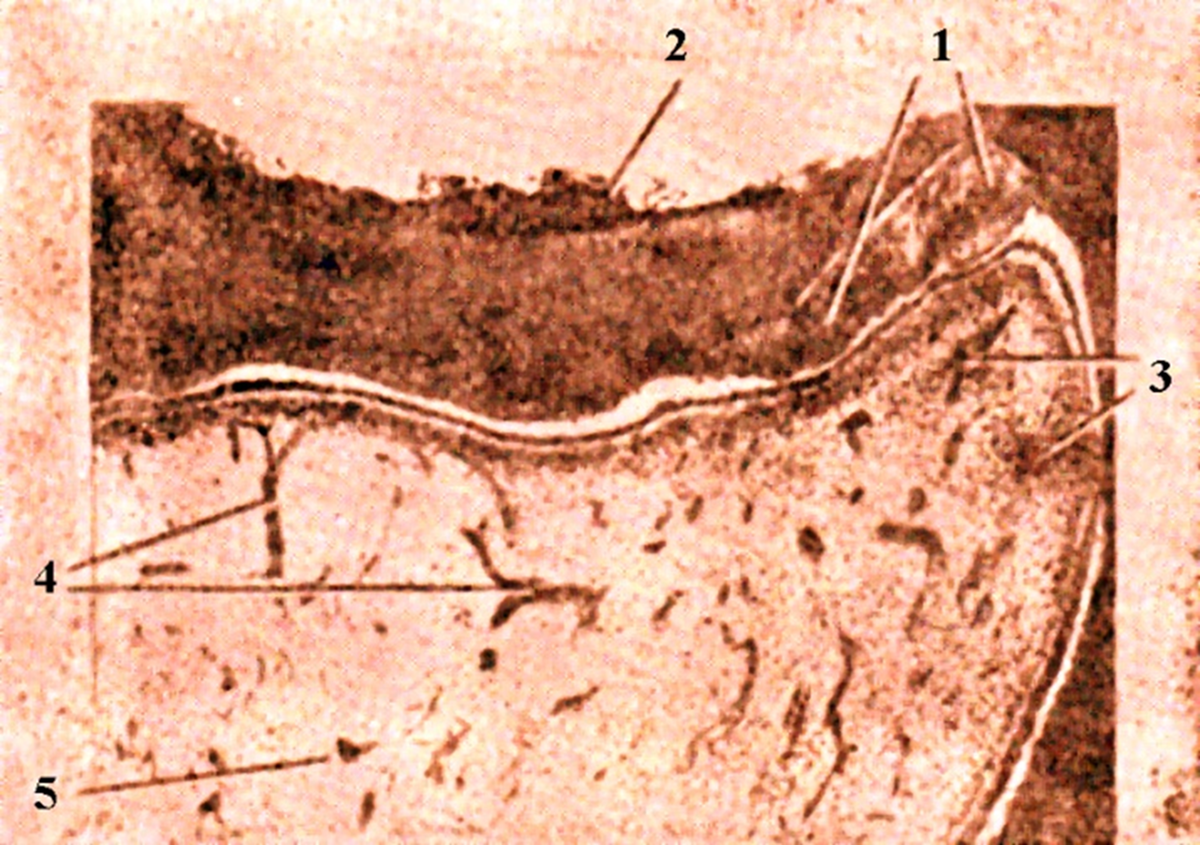
Fig.2.Initial inflammation of the pulp (pulp hyperemia) :
1 – reparative dentin; 2 – demineralized dentin; 3 – single inflammatory cells; 4 – dilated vessels; 5 – non-inflamed pulp.
It is this form of pulpitis that fully corresponds to the concept of “initial pulpitis,” because if the pulp is exposed, there is no need to guess whether it is caries or pulpitis and what is the main cause of the traumatic pulpitis that has developed.Unambiguously, as soon as the integrity of the dentin-pulp complex is violated as a result of opening the pulp and the pulp is in a "stressful state", such a pathology should already be considered pulpar and diagnosed as "pulpitis", not "caries". After all, that is why the pathological process that has penetrated from the pulp chamber into the periapical tissues is already considered a periodontal pathology, and not a pulpar one.You can read more about this in my article “Khidirbegishvili’s Classification of Inflammatory Diseases and Conditions of the Periapical Tissues of the Tooth” (https://dzen.ru/a/ZF8b-kEW72xkS_ZA).
If, after opening the pulp, it is possible to prevent the penetration of microorganisms into the tooth pulp in time through a defect up to 3 mm in size and it is possible to stop bleeding in less than two minutes, then as a result of direct capping of the pulp with therapeutic pads, it will be possible to keep the pulp viable[5].
At the same time, if the pulp was opened during the evacuation of a completely softened infected circumpulpal dentin(non-selective method), then direct capping of the pulp is not recommended, since in this case we do not have an initial inflammation of the pulp in the form of hyperemia, but an already developed inflammation of the pulp complicated by trauma[6]. In this case, if a pulp that has undergone purulent decomposition with the appearance of pus droplets and other destructive processes is objectively detected through the perforation hole, then the diagnosis, despite the absence of pain, definitely shifts towards pulpitis and it is preferable to carry out not amputation, but extirpation treatment of pulpitis – the only reliable method of treating this pathology[1].
If objectively there are no destructive changes in the pulp, it is possible to perform the technique of "pulpotomy’"[7]. However, it is believed that full pulpotomy causes inhibition of dentin development, especially in immature permanent teeth, which can lead to root canal obliteration, while partial pulpotomy helps preserve the cell-rich tissues of the crown pulp to ensure a higher healing potential[7].
At the same time, based on many years of practical activity , would like to note that when performing a partial pulpotomy , it is sometimes difficult to determine the volume of the pulp to be removed. As for the obliteration of the canal with a complete pulpotomy, sometimes, on the contrary, it prevents the penetration of microorganisms into the periapical tissues[7]. In addition, it was proved that morphological changes indicating inflammation or necrosis mainly occurred in the crown pulp, while the root pulp was viable, which indicates the preservation of the root pulp as a result of pulpotomy[8].
It is important to note, however, that with a complete pulpotomy of the coronal pulp, a therapeutic pad is placed on the root pulp, so this technique should be called “direct root pulp capping,” which differs significantly from conventional direct coronal pulp capping not only in the method of execution, but also often in the result of treatment[8].
As for the indirect pulp capping , it is mainly carried out with an unopened tooth pulp, when the softened circumpulpal dentin has not been completely removed (selective method ) and the tooth pulp is separated from the bottom of the prepared cavity by a thin layer of partially demineralized circumpulpal dentin,the removal of which will lead to the opening of the pulp, since the layer of dense dentin is missing[6]. In this case, it is illogical to diagnose initial pulpitis or pulp hyperemia, since once sclerosed and reparative dentin has not been formed, then microorganisms and toxic products of their vital activity have definitely already penetrated into the tooth pulp from infected circumpulpal dentin, as a result of which the pulp is susceptible not to initial, but already chronic inflammation. That is why therapeutic pads are used to eliminate the inflammatory process in the pulp[7].
Thus, indirect capping of the pulp is carried out not in case of pulp hyperemia, but already in case of chronic inflammation of the pulp.
In case of successful exposure of the material of therapeutic pads to the inflamed pulp, the deposition of sclerosed and reparative dentin occurs, which prevents further infection of the pulp[6].Thus, along with direct and indirect pulp capping, direct partial and direct root pulp capping should also be distinguished separately.
Based on this, a rather paradoxical situation arises when, in the WHO classification of pulpitis, the nosology “initial pulpitis” includes pathology with initial inflammation of the pulp (hyperemia), for the treatment of which direct pulp capping is used, and pathology with clearly developed chronic inflammation of the pulp, for the treatment of which indirect pulp capping is used[4].
Clearly, such tactics violate the generally accepted principles of classification in medicine.
In this case, the "initial pulpitis" is certainly correctly referred to as nosology, in which direct capping of the pulp is carried out. However, the situation is more complicated with nosology, the treatment of which involves the selective removal of carious dentin in order to prevent the opening of an already infected and inflamed pulp as a result of partial removal of destroyed circumpulpal dentin(the selective method). In this case, we are talking, of course, about a rather unpredictable pulp pathology, for the treatment of which an indirect capping of the pulp is used in order to prevent the complete transformation of caries into pulpitis[6].
It is definitely unpredictable, since it is impossible to accurately predict whether, as a result of indirect capping of the pulp, it will be possible to definitively prevent the transformation of caries into developed pulpitis, keeping the pulp viable in the carious tooth.That is why in this case it is more logical to make a conditional long-term preliminary diagnosis of “reversible developed pulpitis” (the word “long-term” indicates the duration of determining the treatment result).The word “conditionally” indicates the impossibility of making an accurate diagnosis, since in this case a morphological study is not carried out, it is impossible to use objective pulp data for diagnosis, and the patient’s complaints and the nature of the pain are rather subjective diagnostic parameters[7].
If, after indirect capping of the pulp and applying a temporary seal for some time (several weeks), the patient's complaints completely disappear and the process does not worsen, then, since pulpitis is suspended, it is advisable to put up a conditional diagnosis of "reversible developed pulpitis" or "аrrested pulpitis" (Fig.2)
Fig.2.Objective condition of the carious cavity in reversible developed pulpitis.
The term "reversible" in this nosology indicates not the natural prevention of the transformation of the carious process into pulpitis, but the artificial suspension of already developed pulpitis as a result of the use of indirect pulp capping. If during this time it is not possible to prevent the final transformation of caries into pulpitis and there is exacerbation of the process, then this nosology, depending on the current clinical picture, should be attributed to one of the forms of developed irreversible pulpitis, and not to caries, and especially not to the initial pulpitis.For the treatment of such pathology, complete extirpation of the pulp is most acceptable[9].
Based on all of the above, reversible developed pulpitis should be considered a transitional form between caries and pulpitis, the treatment of which does not always prevent the complete transformation of caries into pulpitis.This approach is also justified by the fact that it becomes possible to justify the legal responsibility of a doctor in the treatment of such a neglected form of caries, since by fixing such a diagnosis and warning the patient in advance of possible complications, the doctor, in case of an exacerbation of the process, relieves himself of legal responsibility if adequate treatment has been carried out.
Thus, when diagnosing reversible developed pulpitis, one of the most important factors is determining the reversibility or irreversibility of inflammation in the pulp tissues, and not the fact of the developed inflammation itself, the development of which can sometimes be stopped due to the reparative properties of the pulp.
Therefore, this circumstance is a key point both in diagnosis and in choosing a treatment method. In this regard, the research of Levin L.G. deserves attention, who found that pulpitis usually becomes irreversible when the pulp has pronounced inflammation with signs of necrosis, which already makes it impossible to use a biological treatment method[10].
Curiously, the use of a selective method for the removal of demineralized softened circumpulpal dentin in the treatment of reversible developed pulpitis causes a fierce confrontation between AAE and ESE [2][3].While American clinicians are against this technique, Europeans strongly advocate the use of this technique due to the alleged reduction in the likelihood of pulp exposure.According to the AAE position, complete removal of softened infected dentin contributes to the successful outcome of treatment of such lesions[2]. From the ESE standpoint, preservation of the pulp affects the viability of the tooth, making it more resistant to destruction, maintaining the ability to restore tissue, preventing various complications, etc. [3].Moreover, according to ESE representatives, soft dentin remains locally only in the projection of the pulp horns, while in the central part of the cavity, carious dentin is removed to a hard, unchanged state.
Experiments on animal teeth have shown that pulp tissue has an innate ability to regenerate if the bacterial film is removed and the tooth is properly repaired (Mjor & Tronstad 1974, Warfvinge & Bergenholtz 1986).Based on this, the modern division of carious dentin into affected and infected is, in principle, rather arbitrary.
In this regard, it is important to note that according to T. Fusayama, carious circumpulpal dentin consists of two layers: an outer and an inner one.The outer layer is unable to remineralize due to direct bacterial infection and destruction of the collagen matrix.The inner layer, which is affected only by bacterial waste products with the integrity of the collagen matrix, is capable of remineralization[11].
However, based on many years of practical experience, I consider it more acceptable to distinguish not two, but three layers of carious circumpulpal dentin[10] :
1.Completely softened necrotic dentin, abundantly
infected with bacteria.
2. Dense, slightly softened demineralized dentin
containing fewer bacteria.
3. Dense, not softened, often pigmented dentin,
painful during processing, in which the content of bacteria
is minimal, up to their possible absence.
Based on this, by completely removing the softened demineralized circumpulpal dentin using a non-selective method, we obtain a prepared cavity with a thin layer of circumpulpal dentin at the bottom, sometimes with signs of pigmentation and slight mineralization (third layer of dentin).Using a selective preparation method, we obtain a prepared cavity with a thin layer of slightly softened demineralized circumpulpal dentin (second layer of dentin).
However, many clinicians suggest that partial removal of softened demineralized dentin may be unjustified due to the already infected pulp[10].Another part of clinicians prefer to leave a part of the softened dentin due to the unpredictability of opening the pulp when removing softened dentin, which can lead to traumatic damage to the pulp and "stress state of the pulp" (Innes et al. 2016).
Incidentally, the idea of leave partially demineralized dentin over the vault of the pulp cavity belongs to the “father of modern dentistry” Pierre Fauchard (1678–1761), who adhered to this tactic due to the fear of exposing the “nerves” in the tooth, which, in his opinion, would lead to tooth extraction.
In this regard, it is difficult to agree with the seemingly experienced clinician Professor Domenico Ricucci, who in his book "Endodontics. Clinical and biological aspects" unequivocally states that the alleged opening of the pulp is not an accident or negligence, but a consequence of insufficient manual skills of the clinician [14?].
Of course, even an experienced clinician, especially when the dense layer of circumpulpal dentin has not been preserved at all, can only predict with a certain degree of probability the possibility of non-opening of the pulp during the excavation of softened circumpulpal dentin.In this regard, I would like to remind Mr. Ricucci of the instructive words of the famous Green Vardiman Black, who said in 1908: "The question often arises whether the pulp will be exposed after the removal of all carious dentin"(a separate article is devoted to inconsistencies in this book by Ricucci)[13].
The debate about selective or non-selective removal of demineralized dentin has not stopped to this day, and in recent years, supporters of selective caries removal have been fiercely opposed by the AAE and especially by Professor Domenico Ricucci, who, at his annual endodontic Endo Sapiens forums, unreasonably agitates clinicians only for the use of non-selective removal of carious dentin[12].
At the same time, the International Consensus Caries Collaboration (a group of 21 experts from 12 countries), which met in Belgium in 2015, concluded that complete removal of carious tissue to hard dentine is an overtreatment, and advocated selective removal of carious tissue.In addition, together with ESE, a new clinical approach for selective caries removal was proposed[3].
The technique consists of removing only the surface layers of soft dentin and leaving carious dentin hard and leathery on the pulp surface.Moreover, the soft dentin is removed with hand tools and using low-speed tips with spherical bores until the underlying dentin becomes solid during probing[3].In this state, isolated bacteria are trapped and actually in a "stressful environment" (Duncan et al. 2019).
Based on many years of practical activity, I would like to note that when treating such lesions and choosing treatment, first of all, attention should be paid to the patient's age, his state of health, the presence of chronic odontogenic intoxication, pronounced periodontitis, the possibility of covering such teeth with orthopedic structures, the patient's solvency, etc. It is these factors that sometimes dictate the choice of treatment tactics and the possibility of using selective and non-selective removal of demineralized dentin, rather than the strict, and sometimes unreasonable, requirements for the use of these AAE and ESE methods[2][3].
In general, the traditional paradigm of using these techniques has a long history.For example, G.W. Black, in his classic text of 1908, argued that "it is better to expose the pulp of the tooth than to leave it covered only with softened dentin"[13]. Based on the above factors, I would add to Black's statement. “in some cases, it is better to expose the dental pulp than to leave it covered with softened infected dentin in order to objectively verify the presence or absence of destructive changes in the pulp and, on this basis, choose a more appropriate treatment method (pulpotomy or pulp extirpation)”.Of course, such tactics help prevent complications associated with the possibility of destructive changes in the alveolar bone![10].
It is important to note that the transformation of caries into pulpitis is sometimes prevented by nature itself even before the treatment of progressive carious lesions as a result of the formation of sclerosed and reparative dentin by the body's defenses, which prevent the penetration of microbes and their waste products from the disintegrated infected circumpulpal dentin into the tooth pulp(Fig.3). In this case, since not all the dentin bridge consists of softened circumpulpal dentin, it is possible to perform non-selective removal of carious dentin, as a result of which the dentin bridge is a dense septum, sometimes slightly mineralised.
Fig.3. Protective and adaptive layers of carious process that caused pulp atrophy.
Such a nosology, although te depth of the lesion corresponds to a reversible developed pulpitis, however, in its treatment there is no longer a need to use an indirect capping of the pulp, since due to the progression of the carious process, layers of sclerosed and reparative dentin have already formed due to the protective forces of the body.Based on this, this pathology should be attributed to caries, not pulpitis, and conditionally called "аrrested dentin caries".
The term «аrrested» in this case indicates a natural suspension of the progressive carious process in the dentin and, accordingly, in the pulp by the body's protective immune forces, rather than the artificial use of therapeutic pads.Based on this, there is no strict need to use indirect pulp capping in the treatment of this nosology[10].
It is important to note that if the dense dentine bridge is quite thin, then protective pads must be used to prevent the traumatic effect of polymerization shrinkage of adhesive systems and composites on the pulp .
Thus, the protective reparative forces of the body are able to prevent not only the progression of caries (arrested caries), but also pulpitis (arrested pulpitis).
Consequently, with the progression of the carious process in the circumpulpal dentin with the integrity of the pulp cavity, three completely different nosologies are diagnosed: “dentin caries”, “arrested dentin caries” and “reversible developed pulpitis”.As for the nosology of "dentin caries", it is diagnosed when the protective adaptive layers of sclerotic and reparative dentin have not formed, but after using a non-selective method, the roof of the pulp cavity consists of a dense, but not mineralized layer of circumpulpal dentin.You can read more about this in my article “Modern clinical classification of caries by Khidirbegishvili” (https://dzen.ru/a/ZF5K_9gNQUkptMnH).
Based on all of the above, the following biological methods of pulp treatment should be emphasised:
• Indirect pulp capping
• Direct pulp capping
• Direct partial pulp capping
• Direct root pulp capping
Indirect pulp capping is mainly performed with the selective removal of carious dentin, when, due to the danger of opening the pulp, the doctor leaves some part of the softened circumpulpal dentin on the dentin bridge. When diagnosing such pathology in the case of a positive outcome of treatment, it is advisable to make a diagnosis of "reversible developed pulpitis"and cover the softened demineralized dentin bridge with a therapeutic pad.
Direct pulp capping is performed when the pulp is accidentally exposed due to trauma to an intact tooth or when preparation dense and uninfected layers of mantle and circumpulpal dentin using a non-selective method.This technique should be performed if the exposed defect is up to 3 mm in size and pulp bleeding can be stopped promptly. This condition should be diagnosed as "incipient pulpitis" or "reversible initial pulpitis," and treatment involves covering the exposed pulp with a therapeutic pad.
Direct partial pulp capping is performed when the pulp has already been exposed by the carious process or exposed during the preparation of softened demineralized dentin using a non-selective preparation method and the size of the exposed defect is more than 3 mm.A prerequisite for carrying out this technique is the timely cessation of bleeding and a visually determined limited inflammatory focus without destructive changes in the pulp.This lesion should be conditionally diagnosed as “reversible partial pulpitis” or “reversible coronal pulpitis”, the treatment of which involves partial removal of the coronal pulp with the application of a therapeutic pad to the remaining coronal pulp.
Direct root pulp capping is performed when the pulp has already been exposed by the carious process or exposed during the preparation of softened demineralized dentin using a non-selective preparation method and the size of the exposed defect is more than 3 mm.A mandatory condition for carrying out this technique is the timely cessation of bleeding and visually determined pronounced destructive changes in the pulp.This type of lesion should be conditionally diagnosed as “reversible complete pulpitis” or “reversible root pulpitis”, in the treatment of which the coronal pulp is completely removed, and a therapeutic pad is placed on the root pulp.
Thus, when diagnosing reversible forms of pulpitis, attention should be paid to the following indicators: sensitivity to hot and cold, spontaneously passing in a few seconds, absence of day and night spontaneous aching pains and pain on percussion, the size of the opening of the pulp cavity and, if it is sufficient, it is necessary to pay attention to the objective condition of the visible area of the pulp and necessarily the intensity bleeding from the pulp.However, it is important to note that reversible and irreversible pulpitis can also be completely painless in 14-60% of cases (Seltzer et al. 1963, Michaelson & Holland 2002).
Particular attention should be paid to bleeding from the pulp, which directly affects not only the diagnosis, but also the outcome of treatment.Excessive bleeding after pulp exposure is usually associated with increased inflammation, which reduces the ability to recover in the area of exposure [5].If pulp bleeding cannot be stopped for a long time, then this indicates the irreversibility of the pulp.If there are no signs of bleeding at all in the affected area, then the pulp tissue is most likely, necrotized.It is important to note that moderate bleeding inside the root canal leads to a constant influx of stem cells, and bacteria and their toxins play a key role in the direct stimulation of pulp cells and stem cells[5].
Depending on the type of pulp exposure, the time to stop bleeding usually varies from 1-3 to 10 minutes. Sometimes bleeding must be stopped by pressing a sterile cotton ball soaked in a solution of sodium hypochlorite, hydrogen peroxide or iron sulfate [5].
Stopping the bleeding is quite important, since a blood clot can prevent the tight contact of the healing pad material with the pulp tissue, which will negatively affect the treatment outcome.
It is also important to pay attention to indirect indicators of the choice of biological
treatment: the age and physical condition of the patient, the degree of destruction of the tooth crown for the use of inlays and anchor pins, the possibility of using the tooth to support a bridge prosthesis or to attach a removable denture clamp, etc..The patient's ability to pay is also an important factor.
Thus, the pulp is completely preserved only with initial pulpitis and reversible developed pulpitis, and in other nosologies the pulp is partially or completely removed.In addition, it is important to note that only the diagnosis of initial pulpitis does not cause any particular difficulties due to the cause of its occurrence and the choice of treatment tactics, although it is also impossible to predict the outcome of treatment of this nosology.
Special difficulties arise in the diagnosis of reversible developed pulpitis, reversible partial pulpitis and reversible complete pulpitis, since it is sometimes difficult to determine the degree of infection and destruction of the crown and root pulp.That is why the diagnosis of reversible forms of pulpitis should always be considered as "preliminary", since it is impossible to be completely sure of the pulp's ability to recover.
For more information on the use of various treatment methods in different forms of pulpitis, see my article "Modern clinical classification of Khidirbegishvili's pulpitis" ( https://dzen.ru/a/ZF5UQ0ej8SbfgCyY), which proposes a new clinical classification of pulpitis, which distinguishes reversible and irreversible forms of pulpitis, as well as special forms of pulpitis :
Reversible pulpitis
• Reversible initial pulpitis(initial pulpitis)
• Reversible developed pulpitis
Reversible рartial pulpitis
• Reversible partial pulpitis(reversible coronal pulpitis
• Reversible full pulpitis( reversible root pulpitis)
Irreversible pulpitis
• Unitary pulpitis
• Hyperplastic pulpitis (pulp polyp)
• Purulent pulpitis (pulp abscess)
• Fibrous pulpitis (fibrosis of the pulp)
• Unspecified pulpitis
Irreversible partial pulpitis
Special forms of pulpitis
• Traumatic pulpitis
• Retrograde pulpitis
• Concremental pulpitis
• Residual pulpitis
• Idiopathic pulpitis
Thus, with the progression of the carious process in the dentin and pulp of the tooth, the following completely different nosologies are diagnosed : "dentine caries", "arrested dentine caries", "initial pulpitis", "reversible developed pulpitis","reversible crown pulpitis", "reversible root pulpitis", "irreversible forms of pulpitis" and "special forms of pulpitis".Moreover, before the opening of the pulp cavity and the formation of irreversible forms of pulpitis, only : "dentine caries", " arrested dentine caries" and "reversible developed pulpitis".
Thus, in order to eliminate the confusion regarding the accessories of these nosologies by various dental schools to caries or pulpitis, it is necessary to finally recognize that only two of them (“dentin caries”, “arrested dentin caries”) refer to caries, and the rest to pulpitis.As for the nosologies "dentine caries" and "arrested dentine caries", can read more about these nosologies in my article "Modern clinical classification of Khidirbegishvili's caries"( https://dzen.ru/a/ZF5NT0EW72xkUWOe).
RESULTS AND DISCUSSION
Unfortunately, there is still no reliable method for accurately assessing the condition of pulps. At the same time, the current method for diagnosing the reversibility or irreversibility of inflamed pulp using biological markers of inflammation has not yet fully proven itself.At the same time , the modern method of diagnosing the reversibility or irreversibility of an inflamed pulp using biological markers of inflammation has not yet fully justified itself. Nevertheless, further studies using more accurate control methods using an autofluorescence diagnostic device (AFS), which allows selectively removing infected dentin by visualizing areas of bacterial invasion, do not stop[10].
As for the factors affecting the healing of the pulp, especially after direct capping of the pulp, they include : bacterial infection,the extent of pulpal bleeding[6],pulp stress situation, operative debris,tunnel defects in dentin bridge , etc [5].As for surgical debris, it includes fragments of dentin from cavity preparation and foreign particles that mix with coating materials. As for tunnel defects in the formed dentine bridge, this is due to the intensity of damage to the pulp and repeated infection of the pulp through these defects that have arisen, communicating with the pulp [5].
It is also important to note that when reparative dentin is deposited on the walls of the pulp cavity, the pulp/ volume decreases, the proportion of collagen increases and the cellular composition decreases, which leads to a decrease in its functions. This condition is called "pulp atrophy" and it is in this condition that the pulp often functions after successful treatment with a biological method of pulp treatment , when sclerosed and reparative dentin has been developed under the influence of a therapeutic pad (Fig.3).
Thus, the inflamed pulp never returns to its original non-inflamed state, however, in a state of atrophy, it can still function in a cured carious tooth. At the same time, it is important to always remember that as a result of the biological treatment method, the pulp can completely mineralize (fibrous pulpitis) or completely necrotize (pulp necrosis),but even in this condition the tooth can function for some time without causing pain or discomfort[10].
At the same time, the use of pulp preservation techniques can eventually lead to its metaplasia into bone or cementum-like tissue, which can cause partial or complete obliteration of the root canal, significantly complicating subsequent endodontic treatment.At the same time, this tissue is permeable to infection and physiologically has little in common with the pulp, since it has lost all those protective and adaptive functions for which we sought to preserve it. Metaplastic pulp, which can function for years, is especially dangerous, because it can cause irreversible changes in bone tissue against the background of apparent well-being[10].On this basis, in controversial situations, especially in teeth used for the support of a bridge prosthesis, it is advisable to depulpate them.
Therefore, the fact that there is no pain should not give the doctor confidence that the process has not progressed to chronic inflammation.Unfortunately, modern science is still powerless to determine when and what will cause the process to worsen.This is why, after vital pulp therapy, the condition of the teeth should be carefully monitored, including a clinical examination after 6 months and radiographic data after 1 year.
CONCLUSION
The proposed methods of biological treatment of pulp and the new classification of pulpitis will help doctors to reliably diagnose the main forms of manifestation of pulp pathology and choose the appropriate treatment methods.At the same time, when using this classification, there are no problems with diagnosis, which cannot be said about some classifications used today.
In conclusion, I invite colleagues to participate in the discussion of the clinical issues raised in the article.I will gratefully accept and take into account all the corrections and recommendations you have sent.
Conflict of interests. The author declare no conflict of interests
Otari Eduardovich Khidirbegishvili is a 1978 graduate of SGMI. More than forty years engaged in practical and scientific-pedagogical activities in the city of Tbilisi. During this time he has published more than 100 articles in leading dental journals, and in 2005 the Stomatological Association of Russia published the monograph ‘Modern Cariesology’, which is accepted for teaching in Russia and in many countries. He is the author of the world's most progressive classifications of caries, pulp diseases, pulpitis and periodontitis, only using which it is possible to make reasonable diagnoses of these major dental diseases! Because of his developments in the field of theoretical dentistry, he is the only Georgian scientist whose picture is on the cover of the prestigious Russian magazine ‘Maestro of Dentistry’ (No. 1(10)2003). Unfortunately, because of his pro-Russian orientation and criticism of some scientific foundations of the Georgian dental school and his desire to create the foundations of this scientific school, he is deprived of scientific regalia by the local professors in his home country!
REFERENCES
1. Borovsky E. V. Therapeutic dentistry. - M.: "Medical Information Agency", 2003. - 840 p.
2.American Association of Endodontists (2013) Endodontic diagnosis. https://www.aae.org accessed 3rd September 2018.
3. Duncan H F, Galler K M, Tomson P L et al. European Society of Endodontology position statement: Management of deep caries and the exposed pulp. Int Endod J 2019; 52: 923-934.
4. World Health Organization. Oral Health Surveys Basic Methods. First Ed., WHO, Geneva, 1971; Fifth Ed., WHO, Geneva, 2013. 125 p.
5.Asgary S., Parhizkar A. Importance of “time” on “haemostasis” in vital pulp therapy. Eur Endod J. 2021;2021(6):128–129. [PMC free article] [PubMed] [Google Scholar]
6.Islam R, Islam MRR, Tanaka T, Alam MK, Ahmed HMA, Sano H. Direct pulp capping procedures - Evidence and practice.Jpn Dent Sci Rev. 2023 Dec;59:48-61.
7. A clinical report on partial pulpotomy and capping with calcium hydroxide in permanent incisors with complicated crown fracture. Cvek M. J Endod. 1978;4:232–237. [PubMed] [Google Scholar]
8. Coronal pulpotomy for cariously exposed permanent posterior teeth with closed apices: a systematic review and meta-analysis. Alqaderi H, Lee CT, Borzangy S, Pagonis TC. J Dent. 2016;44:1–7. [PubMed] [Google Scholar]
9.Bjørndal, Management of deep caries and the exposed pulp, Int. Endod. J., № 52, с. 949.
10..Kochmareva A.S., Makeeva I.M., Shelemetieva G.N., Turkina A.Yu. The use of the autofluorescence diagnostics device for controlled сaries excavation. Stomatology for all. 2024; №1(106): 4—8. doi: 10.35556/idr-2024-1(106)4-8.
11.Fusayama T. 1997. The process and results of revolution in dental caries treatment. Int Dent J. 47(3):157-166. Fusayama T, Kurosaki N. 1972. Structure and removal of carious dentin. Int Dent J. 22(3):401-411.
12. Ricucci D, Loghin S, Siqueira J Jr (2014) Correlation between clinical and histologic pulp diagnoses. Journal of
Endodontics 40, 1932–9.
13.Black GV. The Technical Procedures in Filling Teeth. Vol. 2. Chicago: Medico-Dental Publishing Company; 1908. A Work on Operative Dentistry.
14.Glossary of Endodontic Terms. American Association of Endodontists 2020.pulp-capping materials for permanent teeth. Dent Mater J. 2016;35:1–12..
15. Oral Investig. 2020 Feb;24(2):521-532. doi: 10.1007/s00784-019-03114-5. Epub 2019 Nov 26. PMID: 31773371.
16. Lynch, C.D., O'Sullivan, V.R. and McGillycuddy, C.T., 2006. Pierre Fauchard: the'father of modern dentistry'. British dental journal, 201(12), pp.779-781.
17. Harms CS, Schafer E, Dammaschke T (2019) Clinical evaluation of direct pulp capping with calcium silicate cement - treatment results over an average period of 2.3 years. Clinical Oral Investigations https://doi.org/10.
1007/s00784-018-2767-5.
18.Banerjee A, Kidd EA, Watson TF. 2000. In vitro evaluation of five alternative methods of carious dentine excavation. Caries Res. 34(2):144-150.
19.Transdentinal stimulation of reparative dentine formation by osteogenic protein 1 in monkeys. Rutherford B, Spangberg L, Tucker M, Charette M. Arch Oral Biol. 1995;40:681–683. [PubMed] [Google Scholar]
20. Response of human dental pulp capped with biodentine and mineral trioxide aggregate. Nowicka A, Lipski M, Parafiniuk M, et al. J Endod. 2013;39:743–747. [PubMed] [Google Scholar]
21.Wolters, W.J.; Duncan, H.F.; Tomson, P.L.; Karim, I.E.; McKenna, G.; Dorri, M.; Stangvaltaite, L.; van der Sluis, L.W.M. Minimally invasive endodontics: A new diagnostic system for assessing pulpitis and subsequent treatment needs. Int. Endod. J. 2017, 50, 825–829. [Google Scholar] [CrossRef]