Chest anatomy and stab
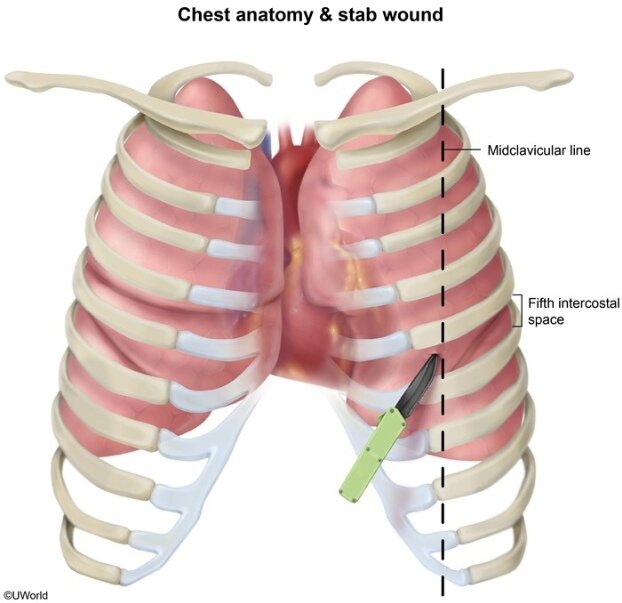
A penetrating, laterally directed stab wound (possibly from a left-handed assaulter) that involves the fifth intercostal space (ICS) at the left anterior midclavicular line (MCL) would most likely injure the left lung. The lungs occupy most of the volume of the thoracic cavity. The apex of each lung extends into the neck (3-4 cm above the first rib). The lung bases are in direct contact with the diaphragm, which separates the right lung from the right lobe of the liver and the left lung from the stomach, spleen, and (occasionally) left lobe of the liver. The mediastinal surface of each lung has a cardiac impression that accommodates the heart.
A deeper (and more medially directed) wound could have injured the left (not the right) ventricle. The heart is located behind the sternum, and its anterior surface is partially covered by the lungs. The cardiac apex is formed by the left ventricle. Depending on heart size, the point of maximal apical impulse can be felt at the fifth left ICS (between the fifth and sixth ribs) at the left MCL. All other heart chambers, including the right ventricle, lie medial to the left MCL and are unlikely to have been affected by the injury. The right ventricle forms the sternocostal (anterior) surface of the heart (Choice E). The diaphragmatic (inferior) surface is formed by the left and right ventricles and is in contact with the central tendon of the diaphragm. The posterior surface of the heart is formed mainly by the left atrium
- The azygos vein lies in the posterior mediastinum immediately to the right of the midline. It drains blood from the posterior intercostal veins into the superior vena cava.
- The inferior vena cava is located in the mediastinum, lies to the right of midline, and drains into the right atrium.
Aortic arch
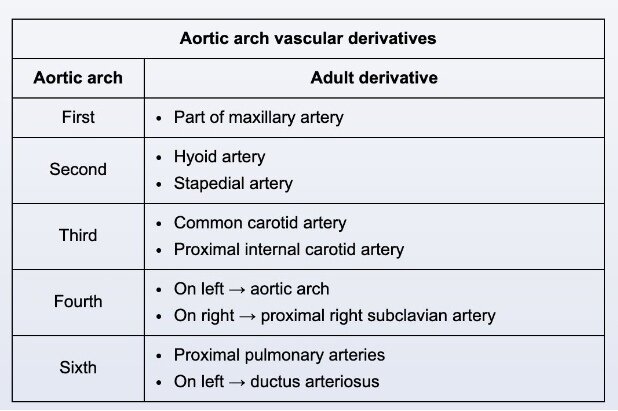
This patient most likely has a patent ductus arteriosus (PDA). The ductus arteriosus is an embryonic derivative of the sixth aortic arch that allows fetal blood to pass directly from the pulmonary artery to the proximal descending aorta (bypassing the pulmonary circulation). This vessel usually closes shortly after birth, secondary to decreased prostaglandin E2 (PGE2) levels and increased oxygen concentration. Patency of the ductus after birth results in a left-to-right shunt that can cause left ventricular volume overload and symptoms of heart failure (eg, failure to thrive, respiratory distress). Physical examination will show a continuous "machinery-like" murmur and palpable thrill over the left infraclavicular region due to turbulent blood flow through the PDA.
Pharmacologic closure of a PDA can be achieved by PGE2 synthesis inhibitors (eg, indomethacin) in premature infants. However, older patients usually require surgical ligation or percutaneous PDA occlusion.
Pulmonary circulation-systemic circulation
In order to maintain blood flow through the body, the blood flow (mL/min) in the pulmonary circulation must closely match the blood flow in the systemic circulation. This is true for conditions of both exercise and rest as the circulatory system is a continuous circuit. If the flow of blood through the pulmonary circulation is less than the flow of blood through the systemic circulation, the left ventricle would soon empty completely. Alternately, if the flow of blood is significantly greater in the pulmonary circulation than it is in the systemic circulation, the left ventricle would soon be overloaded.
The major exception to this is the bronchial circuit, which supplies oxygen and nutrients to the pulmonary parenchyma from the systemic circulation but drains mostly to the left atrium as opposed to the right atrium (creating a right to left shunt that acts as a partially independent circuit). However, this typically accounts for <5% of the systemic cardiac output.
- The arterial oxygen contents of the pulmonary and systemic circulations are dramatically different due to deoxygenated blood in the pulmonary arterial circulation and oxygenated blood in the systemic arterial circulation.
- Although the resistance of the pulmonary vasculature may be increased in some circumstances (eg, high altitudes, idiopathic pulmonary hypertension), the arterial resistance in the systemic circulation is considerably higher in all scenarios.
- The mean arterial pressure, diastolic arterial pressure, and driving pressure for blood flow (difference between mean arterial and venous pressures) are considerably different in the pulmonary and systemic circulations both at rest and during exercise. The normal mean systemic arterial pressure ranges between 70-100 mm Hg and the normal mean pulmonary arterial pressure is approximately 14 mm Hg, whereas venous pressures in both circuits approach 0 mm Hg. Due to the low resistance of the pulmonary circuit, only a small difference between arterial and venous pressures is needed to maintain blood flow compared to the relatively large difference needed between systemic arterial and venous pressures.
Ecg effects of antiarrythemic drugs
Amiodarone is a commonly used antiarrhythmic drug with wide-ranging antiarrhythmic effects and corresponding ECG manifestations. It primarily functions as a class III antiarrhythmic by inhibiting the rapid component of the delayed rectifier potassium current, which is responsible for ventricular repolarization. This prolongs action potential duration and the effective refractory period, suppressing electrical foci that stimulate atrial and ventricular arrhythmias. It also prolongs the QT interval on ECG, which increases the risk of torsade de pointes; however, compared to other class III antiarrhythmics (eg, dofetilide, ibutilide), the risk of torsade de pointes with amiodarone is low.
Amiodarone also has the following effects:
- Class I effect: Amiodarone somewhat inhibits the fast sodium channels responsible for cardiomyocyte depolarization (phase 0). This slows ventricular depolarization to suppress arrhythmogenic foci, and it prolongs QRS complex duration on ECG.
- Class II and IV effects: Amiodarone has beta-blocking properties that inhibit sympathetic stimulation of the conduction system. The drug also inhibits the slow L-type calcium channels responsible for depolarization of the sinus node and atrioventricular node. Both effects prolong the refractory period of the conduction system to suppress arrhythmogenic foci and in doing so contribute to a decreased sinus rate (ie, slowed heart rate) and a prolonged PR interval on ECG.
Decompensated heart failure
This patient's progressive dyspnea, orthopnea, and lower extremity swelling are consistent with acute decompensated heart failure. Heart failure occurs when a structural or functional cardiac disorder impairs ventricular filling or ejection of blood, causing reduced cardiac output and elevated filling pressure. The reduced cardiac output causes an initial drop in blood pressure, which triggers compensatory neurohormonal activity mainly via stimulation of the sympathetic nervous system and renin-angiotensin-aldosterone system (RAAS).
These adaptations function together in an effort to improve organ perfusion by increasing cardiac chronotropy and inotropy (improves cardiac output), promoting arterial and venous vasoconstriction (maintains perfusion pressure), and expanding the extracellular fluid compartment (improves circulating blood volume). However, over time, these responses lead to adverse consequences that perpetuate a downward spiral of progressive cardiac deterioration. Chronic hemodynamic stress (eg, increased preload and afterload) and prolonged exposure to sympathetic drive (catecholamines) and RAAS stimulation (angiotensin II, aldosterone) lead to deleterious remodeling with worsening cardiac function and eventual symptomatic decompensation.
- Ventricular end-systolic and end-diastolic pressures are increased in heart failure due to increased preload and afterload.
- Heart failure triggers the myocardium to secrete natriuretic peptides (ie, atrial natriuretic peptide, brain natriuretic peptide) in response to myocardial stretch from volume
overload. These peptides stimulate vasodilation and increase salt and water excretion to improve the symptoms of heart failure; however, these positive effects are overpowered by the negative effects of increased sympathetic drive and RAAS activation.
Atheletic hearts
This professional athlete most likely has the cardiovascular adaptations of athlete's heart. The soft systolic murmur likely represents a pulmonic flow murmur, a common finding due to the high stroke volume that develops with intensive endurance training.
The adaptations of athlete's heart differ depending on whether intensive endurance training (eg, long-distance running) or resistance training (eg, heavy weightlifting) is pursued. With endurance training, systemic vascular resistance (SVR) is reduced (due to vasodilation in skeletal muscle) and blood volume is increased, leading to increased left ventricular (LV)
volume load. To compensate, LV eccentric hypertrophy (ie, LV wall lengthening) develops, which increases LV cavity size to increase diastolic filling capacity and facilitate increased stroke volume and cardiac output. Right ventricular (RV) cavity enlargement also takes place to increase diastolic filling and accommodate the increase in cardiac output; because the right ventricle and left ventricle are arranged in series and contract at the same rate, RV stroke volume must increase to match LV stroke volume and prevent backup of blood flow.
An increase in stroke volume is maintained at rest and allows for adequate cardiac output at low resting heart rate (eg, <55/min). The anterior location of the pulmonic valve and slightly smaller valve area compared to the aortic valve often create a pulmonic flow murmur due to the high stroke volume. The murmur is best heard at the left second intercostal space in the supine position and may disappear when venous return is decreased with standing.
- Pulmonary vascular capacitance is increased with endurance training, allowing the pulmonary circulation to accommodate high flow while minimizing the afterload on the right ventricle.
- Baseline vagal tone is increased with endurance training, facilitating low resting heart rate.
- Intensive resistance training increases SVR during exercise (due to vascular compression by vigorously contracting muscles), which increases LV pressure load and leads to mild concentric hypertrophy (ie, LV wall thickening). Unlike pathologic concentric LV hypertrophy, the LV cavity remains normal in size and diastolic function is maintained. LV stroke volume and ejection fraction remain normal or are slightly increased, and the right ventricle is unaffected. A flow murmur is not expected.