Kiesselbach plexus
The nasal mucosa is highly vascular and easily irritated by trauma (eg, nose-picking), mucosal dryness, foreign body insertion, and rhinitis (eg, allergy, infection). Epistaxis is very common in children and may be classified as anterior or posterior, depending on the bleeding
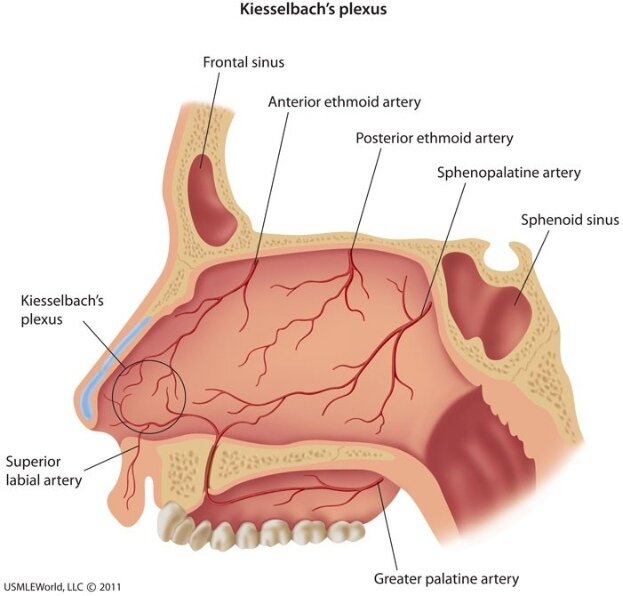
source. Anterior nosebleeds are by far the most common, and the vast majority occur within the vascular watershed area of the nasal septum (anteroinferior part of the nasal septal mucosa) known as Kiesselbach plexus. Anastomosis of the following vessels occurs in this region:
- Septal branch of the anterior ethmoidal artery
- Lateral nasal branch of the sphenopalatine artery
- Septal branch of the superior labial artery (branch of the facial artery)
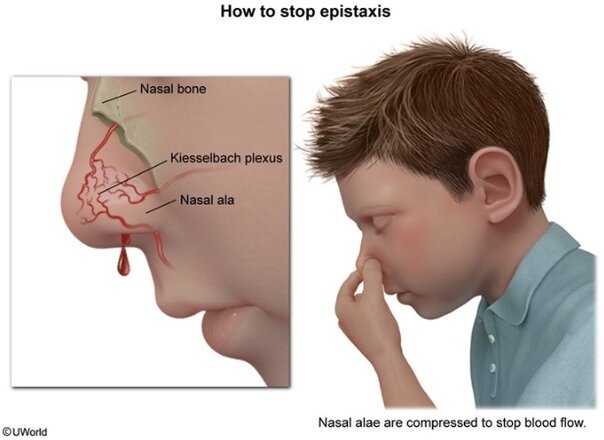
Management is directed at stopping the bleeding from Kiesselbach plexus, preferably by direct compression of the nasal alae. Cautery (eg, silver nitrate) of the area surrounding the bleeding site may be necessary for persistent bleeding.
(Choices A and B) The lateral nasal wall contains the superior, middle, and inferior turbinates (also known as conchae). These 3 bony projections are covered with mucous membrane; they warm, humidify, and filter inspired air and expand and contract in response to environmental changes (eg, temperature, humidity, allergens). The turbinates form corresponding meatuses that serve as drainage pathways. The superior meatus provides drainage for the sphenoidal and posterior ethmoidal sinuses. The middle meatus drains the frontal, maxillary, and anterior ethmoidal sinuses and is the most common site of nasal polyps. The inferior meatus drains the nasolacrimal duct.
(Choices D and E) Branches of the sphenopalatine artery supply the posterolateral wall and posterior choanae. These posterolateral branches are the most likely source of posterior nosebleeds. Posterior epistaxis is usually severe and cannot be treated with cautery.
Allergic conjunctivitis
This patient has nasal congestion, sneezing, and rhinorrhea accompanied by
conjunctivitis. This is consistent with allergic rhinoconjunctivitis, a type 1 hypersensitivity that triggers an allergic response via the binding of a previously recognized antigen to IgE antibodies on mast cells.
Because exposure to allergens results in a rapid allergic response and avoidance of allergens improves symptoms, patients can often distinguish patterns to their reactions. Typical patterns include the following:
- Seasonal variation: The variation is often related to specific pollinators at particular times of the year.
- Geographical variation: Symptoms improve when patients are not exposed to the typical allergens of the region (eg, going on vacation).
- Animal exposure: Symptoms occur when visiting a house with pets or begin shortly after animal acquisition.
- Indoor versus outdoor: Patients with predominantly indoor symptoms may have an allergy to dust mites; outdoor symptoms suggest pollinators.
(Choice A) An allergic reaction to soy products can cause nasal and ocular
symptoms. However, it also typically includes a rash, swelling or itching of the mouth and lips, and/or gastrointestinal symptoms. In addition, it most commonly presents in early childhood when soy is introduced into the diet.
(Choice C) Rhinitis symptoms caused by exposure to cold air are classically associated with nonallergic or vasomotor rhinitis. Nonallergic rhinitis typically does not cause conjunctivitis symptoms.
(Choice D) Tobacco smoke is a respiratory irritant that can worsen symptoms of allergic rhinitis; however, tobacco allergy is rare, and depending on route of intake, would likely produce significant oral (eg, mouth itching/swelling) and pulmonary (eg, asthma) symptoms.
(Choice E) Like allergic rhinitis, medication allergies can be type 1 hypersensitivity reactions. However, these allergies typically present with an urticarial rash shortly after ingestion of the medication; eye symptoms are uncommon.
Rinne test
Hearing loss is classified as either conductive (impaired transmission of air vibrations to inner ear) or sensorineural (involving the cochlea or auditory nerve). The Rinne and Weber tests can be used to help determine the type of hearing loss.
The Rinne test compares air versus bone conduction (via the mastoid bone). As the vibration of the tuning fork fades, air-conducted sound is normally louder and heard longer than bone- conducted sound. The Rinne test is considered positive (normal) if the sound is heard best at the external auditory meatus (air conduction) and negative (abnormal) if the patient hears the vibration better at the mastoid (bone conduction).
- Bone conduction greater than air conduction suggests conductive hearing loss.
The Weber test is performed by placing a vibrating tuning fork on the middle of forehead equidistant from both ears. The vibration carried by bone conduction is normally heard equally in both ears; vibration heard louder in one ear is abnormal.
- Conductive hearing loss causes lateralization to the affected ear as the conduction deficit masks the ambient noise in the room, allowing the vibration to be better heard.
- Sensorineural hearing loss causes lateralization to the unaffected ear as the unimpaired inner ear can better sense the vibration.
The Rinne test is abnormal in this patient's left ear, and the Weber test lateralizes to her left ear. These findings suggest conductive hearing loss in the left ear.
carcinoma
Most carcinomas, including head and neck squamous cell carcinoma, spread first from the primary site of the tumor to regional lymph nodes via the lymphatics. In this patient with a tonsillar squamous cell carcinoma, this spread would be to the upper anterior cervical (ie, jugular) lymph nodes. Assessment of regional lymph node status is important for tumor staging based on the TNM staging system, which evaluates the size and characteristics of the Tumor, regional lymph Node involvement, and distant Metastases.
(Choice A) Similar to the tonsils, adenoid tissue is also lymphatic tissue in the head and neck that can harbor a primary site of head and neck squamous cell carcinoma. However, it is located in the nasopharynx rather than the oropharynx. The spread of cancer is typically to regional lymph nodes rather than to other mucosal sites in the head and neck.
(Choices B, C, and F) Although these are possible sites of distant cancer metastases, they are less commonly associated with metastatic head and neck cancer. Common primary sources for metastases to these sites include:
- Adrenal gland metastases: breast cancer, renal cell carcinoma, and melanoma
- Brain metastases (gray-white matter junction): lung cancer
- Vertebral body metastases: prostate cancer
However, the first site of spread of most carcinomas (including head and neck cancer) is the regional lymph nodes.
(Choice E) The lung parenchyma is the most common site for distant metastases from head and neck cancer. However, regional lymph node spread is typically seen first.
Vagus nerve
The majority of the external ear receives cutaneous innervation from the great auricular nerve, lesser occipital nerve, and auriculotemporal nerve. Most of the external auditory canal, including the external portion of the tympanic membrane, is innervated by the mandibular division of the trigeminal nerve (cranial nerve [CN] V3) via its auriculotemporal branch.
However, the posterior part of the external auditory canal, as well as the concavity and posterior eminentia of the concha, is innervated by the small auricular branch of the vagus nerve (CN X). This patient has experienced vasovagal syncope after stimulation of his posterior external auditory canal by an otoscope speculum. In this form of syncope, parasympathetic outflow via the vagus nerve leads to decreased heart rate and blood pressure.
(Choice A) The accessory nerve (CN XI) provides voluntary motor innervation to the trapezius and the sternocleidomastoid.
(Choice B) The facial nerve (CN VII) has a small motor component to the stapedius and muscles behind the ear. It supplies cutaneous sensation to a small area of the auricle, but stimulation here would be unlikely to trigger a vasovagal response.
(Choice C) The mandibular branch of the trigeminal nerve carries sensation from the majority of the external auditory meatus, except for the posterior wall.
(Choice E) The vestibulocochlear nerve (CN VIII) mediates hearing and vestibular proprioception. It does not mediate any cutaneous sensation.
Squamous cell carcinoma
This patient with dysphagia, a base of tongue mass, and cervical lymphadenopathy likely has mucosal head and neck squamous cell carcinoma (HNSCC). HNSCC arises from the mucosa of the upper aerodigestive tract after accrual of multiple somatic mutations, often caused by the mutagens found in tobacco. Other risk factors for HNSCC include age >40, alcohol use, and immunocompromised status. There has also been a dramatic increase in HNSCC due to human papillomavirus (HPV), which may be seen in younger, nonsmoking patients.
Characteristic pathologic findings of HNSCC include nests and sheets of polygonal cells with abundant eosinophilic cytoplasm that invade the submucosa and surrounding
structures; intercellular bridges and keratin pearls (ie, foci of keratinization) may be seen on light microscopy.
(Choice A) Squamous papillomas are benign tumors that have fibrovascular cores surrounded by squamous epithelium. They can occur in the mucosa of the upper aerodigestive tract but would not spread to regional lymph nodes as they are not malignant.
(Choice B) Adenocarcinomas arise due to mutation of glandular cells and often retain glandular features and some glandular functions, including the production of mucin. The mucosa of the head and neck is made of stratified squamous cells; therefore, cancers arising from this region often retain some features of squamous cells (eg, production of keratin).
(Choice C) Oral candidiasis (ie, thrush) often has an inflammatory infiltrate with pseudohyphae and can present with oral lesions. However, oral candidiasis characteristically appears as white plaques on an erythematous base throughout the mucosa. It does not form a palpable mass or cause firm cervical adenopathy.
(Choice E) Although non-Hodgkin lymphoma, such as follicular lymphoma (characterized by nodular proliferation of lymphocytic follicles), can rarely present in a tonsil, it is unlikely to occur in the base of tongue and is overall much less common than HNSCC, especially in a patient age >60 with a long history of tobacco use.