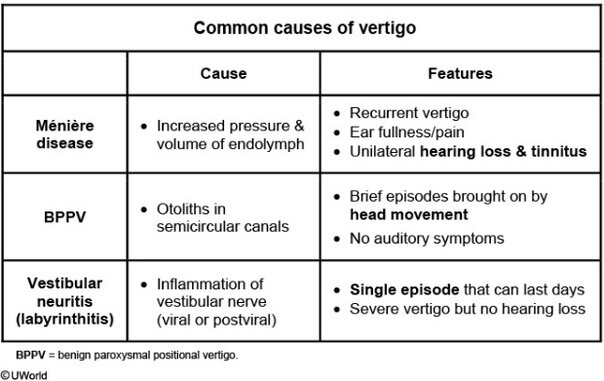
This patient has Ménière disease, a disorder of the inner ear characterized by increased volume and pressure of endolymph (endolymphatic hydrops) that is thought to be due to defective resorption of endolymph. The resultant distension of the endolymphatic system causes damage to the vestibular and cochlear components of the inner ear. Ménière disease is characterized by the following triad:
- Low-frequency tinnitus, or ringing, in the affected ear, often accompanied by a feeling of fullness
- Vertigo, the subjective sensation of spinning or motion in the absence of actual motion; commonly associated with lightheadedness, nausea, and vomiting
- Sensorineural hearing loss, which is variable in severity but usually worsens over time
(Choice A) Multiple sclerosis (MS) is characterized by patchy demyelination in the central nervous system that varies over time. The presentation of MS is highly variable and may resemble Ménière disease, but most patients will have additional, extra-auditory symptoms (eg, visual symptoms, sensory disruptions).
(Choice C) Labyrinthitis is inflammation of the vestibular nerve that causes acute-onset vertigo, nausea, and vomiting. It usually occurs in a single episode following a viral syndrome.
(Choice D) A mass lesion at the cerebellopontine angle is most commonly an acoustic neuroma (schwannoma of CN VIII). An acoustic neuroma could cause sensorineural hearing loss, vertigo, and tinnitus, but symptoms would be persistent and progressive rather than episodic.
(Choice E) Otosclerosis is an inherited condition seen in middle age. Patients present with conductive hearing loss due to bony overgrowth of the footplate of the stapes. Vertigo does not occur.
Thyroglossal duct cyst
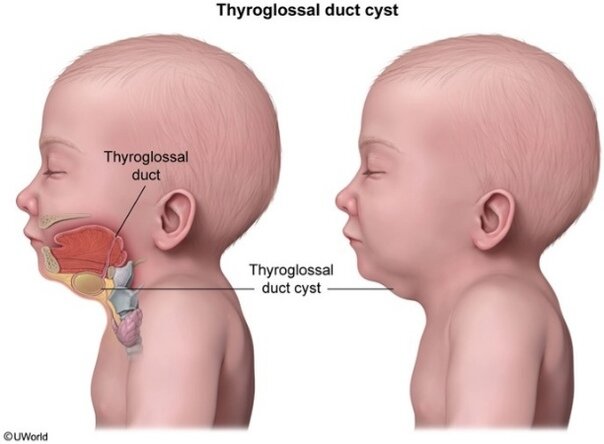
This patient has a thyroglossal duct cyst (TDC), which presents as a midline mass that characteristically moves superiorly with protrusion of the tongue or swallowing. A TDC is often detected when it becomes secondarily infected after an upper respiratory tract infection, leading to erythema and tenderness. It may also be noted incidentally during evaluation of throat or neck symptoms.
The thyroid gland is formed as an outpouching from the pharyngeal epithelium at the base of the tongue. It then descends to the base of the anterior neck via the thyroglossal duct, which extends from the foramen cecum on the dorsal surface of the tongue to the superior border of the thyroid isthmus. If the duct fails to atrophy normally, a TDC can develop from the epithelial remnants within the duct. Because the tract connects to the base of the tongue, protrusion or swallowing causes the TDC to move superiorly. Ectopic thyroid tissue may also form and can reside anywhere along the thyroglossal duct's path.
(Choice A) A paraganglioma is a neuroendocrine tumor that arises from extraadrenal, autonomic paraganglia (eg, carotid body paraganglia) due to the abnormal migration of neural crest cells. Carotid body paragangliomas typically present as lateral neck masses.
(Choice B) Cervical implantation of thymic tissue can result in ectopic thymic cysts, which are rare lesions that may develop along the descent of the thymus (angle of the jaw to the mediastinum). They are typically unilateral (left more often than right) rather than midline.
(Choice C) A cystic hygroma results from abnormal lymphatic development, leading to dilated lymphatic vessels. It presents at birth as a soft mass at the posterior base or lateral aspect of the neck. It would not typically be at the midline or rise with swallowing.
(Choice E) A branchial cleft cyst is an embryologic remnant of branchial arch structures that presents as a lateral (rather than midline) neck mass. A sinus tract or fistula may also be present.
(Choice F) Trapping of skin structures (eg, hair follicles, sebaceous glands) along embryonic fusion lines results in the formation of a dermoid cyst within the subcutaneous tissue. It presents as a midline neck mass but, in contrast to this patient's neck mass, does not move with tongue protrusion or swallowing.
cholestoma
Cholesteatomas are collections of squamous cell debris that form a round, pearly
mass behind the tympanic membrane in the middle ear. They can occur congenitally or may develop in adults as either an acquired primary lesion or secondary to infection, trauma, or surgery of the middle ear. Primary cholesteatomas are a result of chronic negative pressure in the middle ear causing retraction pockets in the tympanic membrane that become cystic; as the squamous cell debris accumulates, a cholesteatoma is formed. Secondary cholesteatomas occur after squamous epithelium migrates to or is implanted in the middle ear ("skin in the wrong place").
Cholesteatomas most commonly cause painless otorrhea. They also can produce lytic enzymes and are often discovered when they erode through the auditory ossicles, causing conductive hearing loss. If a mass grows sufficiently large, it can erode into the vestibular apparatus or facial nerve, causing vertigo or facial palsies.
(Choice A) Cholesterol granulomas can form in the middle ear after hemorrhage but are much less common than cholesteatomas. They appear as bluish-black gelatinous material behind the tympanic membrane. Despite what the name implies, cholesteatomas do not contain any lipid or cholesterol components.
(Choice B) A facial nerve neuroma can grow in the middle ear as the facial nerve courses through this territory. However, it would present with unilateral facial paralysis.
(Choice C) Squamous cell carcinoma is the most common malignant tumor of the ear canal. It typically appears as an ulcerated plaque or nodule. The most common symptom is local or regional pain.
(Choice D) Granulomatous disease of the ear can occur but is uncommon and usually develops in conjunction with a systemic disease, such as sarcoidosis, granulomatosis with polyangiitis, or Langerhans cell histiocytosis.
Alpha agonist
Vasoconstriction by α-adrenergic agonists is prominent in the vessels of the nasal mucosa, making these medications effective decongestants. Phenylephrine, xylometazoline, and oxymetazoline are used as topical preparations for the treatment of allergic rhinitis and common cold associated congestion and rhinitis.
These medications, however, are characterized by rapidly declining effect after a few days of use. This phenomenon is called tachyphylaxis. It occurs because of decreased production of endogenous norepinephrine from the nerve terminals due to a negative feedback mechanism, resulting in relative vasodilation (ie, removal of normal vasoconstrictive tone) and subsequent edema and congestion. This leads to exacerbation of the nasal congestion
symptoms. Rebound rhinorrhea (ie, rhinitis medicamentosa) is described as nasal congestion without cough, sneezing, or postnasal drip. Rhinorrhea may or may not be present (note the paradox in naming). Rebound rhinorrhea is associated with the use of topical decongestants for > 3 days. The use of adrenergic agonists should be stopped to allow the restoration of normal norepinephrine feedback pathways.
Another medication associated with the phenomenon of tachyphylaxis is nitroglycerine. The decrease in its effect is explained by the diminished release of NO from the target cells. Drug- free intervals of 8–10 hours should be maintained during the use of nitroglycerine to prevent tachyphylaxis.
(Choice B) Ephedrine is an indirect-acting adrenergic agonist used as a decongestant. Like the other adrenergic medications, it causes tachyphylaxis after a few days of treatment. A switch to ephedrine would not improve this patient’s rebound rhinorrhea.
(Choice C) This patient has been excessively using a decongestant; if he discontinues it and experiences excessive withdrawal symptoms, a short-term course of topical corticosteroids can be considered for symptom control. However, oral corticosteroids would not be indicated.
(Choice D) Antihistamines are used for the treatment of allergic rhinitis, but they are not effective in treating rebound rhinorrhea.
(Choice E) Antibiotics are effective in the treatment of certain bacterial infections. They are not used in the treatment of rebound rhinorrhea.
Pieree robin sequence
This patient has a small mandible, posteriorly displaced tongue, and U-shaped cleft palate, which is consistent with Pierre Robin sequence. A sequence occurs when a single developmental defect causes a cascade of additional malformations.
In Pierre Robin sequence, hypoplasia of the mandibular prominence leads to micrognathia. Severe micrognathia causes posterior displacement of the tongue (glossoptosis), which blocks fusion of the palatine shelves, resulting in a cleft palate that is characteristically U-shaped. Difficulty breathing occurs because the tongue prolapses into the posterior oropharynx, blocking airflow. Breathing improves when the patient is in a prone position because gravity pulls the tongue anteriorly, opening the airway.
(Choice A) An association is a collection of malformations that are often seen together and do not have a known, common cause (eg, VACTERL association).
(Choice B) A disruption occurs when an external insult (rather than a genetic defect) interrupts and arrests normal fetal development (eg, when an amniotic band disrupts limb
development). No specific external insult has been linked to Pierre Robin sequence, and most cases result from genetic abnormalities.
(Choice C) Genomic imprinting is a normal process that refers to selective activation of gene expression depending on the parent of origin. Aberrant imprinting occurs with uniparental disomy (ie, when a person receives 2 copies of a chromosome from the same parent and no copy from the other parent). Prader-Willi syndrome and Angelman syndrome (15q) are examples of conditions caused by dysfunctional imprinting.
(Choice E) A syndrome is a collection of malformations that have a common cause but are not related anatomically. For example, upslanting palpebral fissures, atrioventricular canal defect, and single palmar crease are all due to trisomy 21.
Cleft lip
The lip and palate form during the fifth-sixth week of embryonic development through a series of fusions:
- The first pharyngeal arch splits into the upper maxillary prominence and the lower mandibular prominence.
- Fusion of the 2 medial nasal prominences forms the midline intermaxillary segment. The intermaxillary segment will become the philtrum of the upper lip, the 4 medial maxillary teeth, and the primary palate.
- The left and right maxillary prominences then fuse with the midline intermaxillary segment to form the upper lip and primary palate. If one of the maxillary prominences fails to fuse with the intermaxillary segment, a unilateral cleft lip results. If both maxillary prominences fail to fuse with the intermaxillary segment, bilateral cleft lip results.
(Choice A) Failure of the medial nasal prominence to fuse and form the intermaxillary segment is associated with severe midline defects, such as holoprosencephaly.
(Choice C) During the seventh-eighth week of embryonic development, the maxillary prominences give rise to palatine shelves. The thin sheets of tissue that comprise the palatine shelves grow medially and fuse into the secondary palate. Fusion of the secondary palate with the posterior aspect of the primary palate forms the complete palate. Failure of any of these processes can lead to cleft palate. The presence of a cleft lip increases the risk of cleft palate, but either can occur in isolation.
(Choice D) The orbits normally arise from the sides of the face and rotate medially. However, excessive tissue from the frontal nasal prominence could result in orbital hypertelorism (wide-set eyes) in addition to a broad forehead and wide nasal bridge.
(Choice E) Micrognathia is characterized by hypoplasia of the mandibular prominence. In Pierre-Robin sequence, the severe micrognathia results in posterior displacement of the tongue (glossoptosis) and prevents fusion of the secondary palate (cleft palate).