Age related macular degeneration
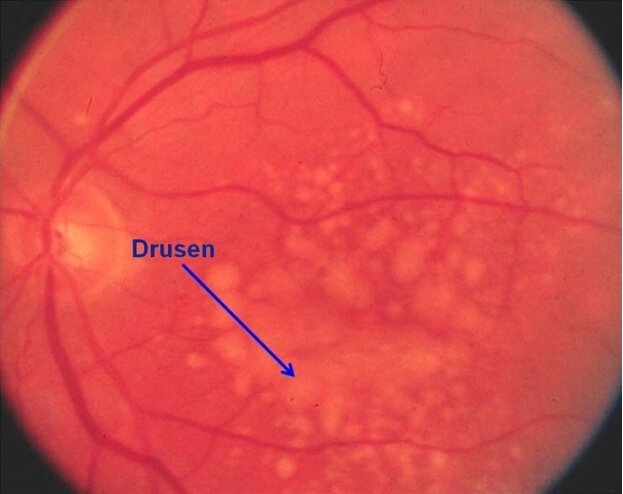
This patient likely has age-related macular degeneration (AMD), the leading cause of blindness in industrialized countries. AMD occurs in genetically predisposed individuals as a result of advancing age and environmental factors (eg, smoking) and is classified into dry and wet subtypes. Dry AMD is characterized by gradual vision loss in one or both eyes and can cause difficulty with driving/reading. The condition likely results from chronic oxidative damage to the retinal pigment epithelium and choriocapillaris, leading to subretinal inflammation with abnormal extracellular matrix formation (eg, confluent drusen, basement membrane thickening). These changes appear on funduscopy as subretinal drusen deposits with pigment abnormalities.
Progressive extracellular matrix accumulation can eventually result in retinal hypoxia, which stimulates local vascular endothelial growth factor (VEGF) production and causes subretinal neovascularization with formation of leaky vessels. This condition is termed wet AMD and presents with acute vision loss (days to weeks) with metamorphopsia (distortion of straight lines). Funduscopy shows a grayish-green subretinal discoloration with adjacent fluid/hemorrhage.
Patients with dry or wet AMD may benefit from antioxidant vitamins and zinc, and smokers should receive smoking cessation counseling to prevent disease progression. Wet AMD usually requires specific treatment with VEGF inhibitors (eg, ranibizumab, bevacizumab).

(Choice A) Therapy against the CD20 glycoprotein on B cells (eg, the monoclonal antibody rituximab) is used to treat various lymphomas and active rheumatoid arthritis.
(Choice B) Epidermal growth factor receptor inhibitors (eg, erlotinib, gefitinib) are used to treat advanced non-small cell lung cancer.
(Choice C) Anti-interleukin-2 therapy is primarily used for immunosuppression in organ transplant patients and in conditions such as graft versus host disease.
(Choice D) Inhibitors of tumor necrosis factor-alpha are used in many inflammatory autoimmune conditions, such as rheumatoid arthritis, inflammatory bowel disease, and seronegative spondyloarthropathies.
Diabetic retinopathy
This patient, with painless vision loss and retinal neovascularization, has proliferative diabetic retinopathy (DR). DR is a result of chronic hyperglycemic injury to the small retinal vessels and is considered a microangiopathic complication of diabetes (along with neuropathy and nephropathy). The prevalence of DR is proportionate to the duration of diabetes and severity of hyperglycemia over time; tight control of diabetes is associated with a lower long-term risk of DR.
DR is categorized as follows:
- Nonproliferative (early disease): The earliest morphologic changes include thickening of the basement membrane and failure of the blood-retinal barrier. Increased permeability allows leakage of fluid into the retina (macular edema), which can distort vision and leave behind lipid-rich deposits (hard exudates). Arteriolar obstruction causes ischemic injury to the retina, which manifests as cotton-wool spots. Other findings include microaneurysms and dot-blot hemorrhages (due to microaneurysm rupture).
- Proliferative (advanced disease): Progressive retinal ischemia stimulates production of angiogenic factors (eg, vascular endothelial growth factor), leading to formation of new retinal vessels (neovascularization). The new vessels are fragile and often extend into the adjacent vitreous. Traction from the vitreous can cause detachment of the retina or laceration of the vessels, leading to acute hemorrhage and vision loss
(Choice A) Age-related macular degeneration presents with slowly progressive central vision loss. It is due to oxidative damage to the pigment epithelium and choriocapillaris with abnormal extracellular matrix formation (drusen). In late-stage disease, patients may develop neovascularization ("wet" macular degeneration), but associated findings include subretinal drusen and pigment abnormalities.
(Choice C) Open-angle glaucoma is a form of optic neuropathy, characterized by ganglion cell death in association with elevated intraocular pressure. It causes insidious loss of peripheral vision; examination findings include enlargement of the retinal cup and a pale optic disc with thinning of the rim.
(Choice D) Atheroembolic retinal artery occlusion presents with acute monocular vision loss. Examination findings include retinal pallor and a cherry red spot at the macula.
(Choice E) Hypertensive retinopathy can manifest with retinal hemorrhages, cotton-wool spots, and hard exudates. However, the thickened and stiffened arterial walls are typically visible as arteriolar narrowing and impingement on the veins where they are crossed by arteries (arteriovenous nicking).
Pupillary asymmetry
This patient has anisocoria (ie, pupillary asymmetry), which indicates a unilateral defect in input from either the ocular sympathetic (pupil dilation) or parasympathetic (pupil constriction) pathway. In response to dim light, input from the oculosympathetic pathway initiates pupillary dilation, allowing more light to reach the retina. Under bright light, parasympathetic input from the ipsilateral oculomotor nerve (CN III) initiates pupillary constriction, limiting the amount of light received by the retina.
Determining which pathway is affected in anisocoria can be accomplished by observing the change in pupillary discrepancy in both bright and dim light:
- Asymmetry that increases in dim light indicates that the smaller pupil is unable to dilate (ie, miosis) due to loss of sympathetic nerve input. Under bright light, the asymmetry will decrease because parasympathetic input (pupillary constriction) is unaffected.
- Asymmetry that increases under bright light indicates that the larger pupil is unable to constrict (ie, mydriasis) due to loss of parasympathetic nerve input. In dim light, the asymmetry will decrease because sympathetic input (pupillary dilation) is unaffected.
This patient has increased asymmetry in a dim room, indicating that the smaller (right) pupil is unable to dilate due to loss of sympathetic nerve input secondary to a lesion in the right oculosympathetic pathway.
(Choices A and D) An oculomotor nerve lesion would disrupt parasympathetic innervation of the ipsilateral pupil, resulting in anisocoria that increases under bright light because the abnormal larger pupil is unable to constrict in response to light.
(Choice B) Damage to the left oculosympathetic pathway would cause loss of sympathetic input to the left eye, resulting in a fixed, constricted pupil in the left eye (with increased asymmetry in dim light) rather than in the right.
(Choices C and F) The optic nerves carry the afferent portions of the pupillary reflex from each eye. A unilateral optic nerve lesion would not cause pupillary asymmetry, but instead monocular vision loss and decreased bilateral pupillary constriction in response to light entering the affected eye (ie, relative afferent pupillary defect).
Internuclear opthalmoplegia
This patient has internuclear ophthalmoplegia, a disorder of impaired horizontal gaze caused by damage to the medial longitudinal fasciculus (MLF). The frontal eye field initiates horizontal gaze through the contralateral abducens (CN VI) nucleus, which communicates with the ipsilateral oculomotor (CN III) nucleus by way of the MLF. This allows for simultaneous activation of the lateral rectus muscle in the contralateral eye (abduction) and the medial rectus muscle in the ipsilateral eye (adduction), resulting in coordinated conjugate horizontal gaze.
Unilateral MLF lesions typically occur in older patients with lacunar strokes in the dorsal pons or midbrain (pontine artery distribution) and result in impaired adduction of the ipsilateral eye during horizontal gaze, causing diplopia. Abduction in the contralateral eye is preserved (but often with gaze-evoked nystagmus). The pathways for convergence and the pupillary light reflex bypass the MLF lesion, so these reflexes are generally preserved.
(Choice A) The abducens nerves innervate the lateral rectus muscles, which abduct the eyes. A lesion involving an abducens nerve would result in impaired abduction of the ipsilateral eye due to lateral rectus muscle palsy.
(Choice B) The lateral geniculate nucleus is located in the thalamus and relays visual information to the ipsilateral primary visual cortex. Damage to this structure would result in a contralateral homonymous hemianopia.
(Choice D) Unilateral infarction of the primary visual cortex in the occipital lobe (eg, posterior cerebral artery occlusion) typically results in contralateral homonymous hemianopia with macular sparing as the macula receives collateral circulation from the middle cerebral artery.
(Choice E) Oculomotor nerve palsy (eg, ipsilateral mydriasis, ptosis, "down and out" deviation of the eye) may occur with microvascular nerve ischemia (eg, diabetes mellitus) or nerve compression (eg, posterior communicating artery aneurysm).
(Choice F) The superior colliculus controls vertical gaze. Damage to the superior colliculus in the dorsal midbrain causes Parinaud syndrome (eg, upward gaze palsy, absent pupillary light reflex, impaired convergence).
CMV
Patients with untreated AIDS who have CD4 counts <50/mm3 are at high risk for cytomegalovirus (CMV) retinitis. Suspicion is often raised when a patient with advanced AIDS develops slowly progressive blurred vision, scotoma (blind spots), floaters, or photopsia (flashing lights). Although most cases are thought to arise due to hematogenous dissemination of CMV, serum testing for the virus is often (~50%) negative. Therefore, the diagnosis is typically established when funduscopy reveals yellow-white, fluffy retinal lesions near the retinal vessels associated with hemorrhage.
Treatment is required to prevent progression and blindness. Ganciclovir, a guanine nucleoside analogue that is structurally similar to acyclovir but expresses greater activity against CMV DNA polymerase, is first-line therapy. Patients are also typically started on antiretroviral therapy to increase CD4 count. A major complication of CMV retinitis is retinal detachment due to the replacement of damaged retina with thin, atrophic scar tissue (which is prone to tear).
(Choice A) Acyclovir is used to treat herpes simplex (HSV) and varicella zoster virus (VZV) infections. Although these infections occasionally cause acute retinal necrosis, most cases arise in older, immunocompetent individuals (not patients with advanced AIDS). In addition, HSV retinitis and VZV retinitis are usually associated with significant vitreal inflammation, spotty peripheral retinal lesions, and infrequent hemorrhage.
(Choice B) Candida endophthalmitis is treated with amphotericin B. Funduscopy usually reveals focal, white, mound-like lesions on the retina. Most cases occur in the setting of an indwelling central venous catheter or total parenteral nutrition.
(Choice C) Clarithromycin is used in conjunction with other antibiotics for the treatment of Mycobacterium avium complex infection, which usually causes fever, night sweats, abdominal pain, and diarrhea.
(Choice D) Cryptococcus neoformans infections are treated with flucytosine, a fluorinated analog of cytosine, in combination with amphotericin B. Although cryptococcal endophthalmitis can occur in patients with advanced AIDS, it is much less common than CMV retinitis, and patients often have other manifestations of cryptococcal infection such as skin lesions or meningoencephalitis.
(Choice F) Penicillin G is used to treat ocular (and neuro-) syphilis. Ocular syphilis often presents as uveitis but can cause retinitis, which usually appears as ground-glass lesions with significant vitreal inflammation. Most patients also have manifestations of syphilitic meningitis (eg, headache, vomiting).
Glaucoma
Aqueous humor is secreted by epithelial cells of the ciliary body into the posterior eye chamber. The fluid then flows through the pupil into the anterior chamber to the iridocorneal angle. Here, it diffuses through a trabecular network into Schlemm's canal (scleral venous sinus) and subsequently drains into episcleral and conjunctival veins. A small amount of aqueous can also diffuse through the ciliary muscle and adjacent sclera (uveoscleral pathway).
Open-angle glaucoma is characterized by increased intraocular pressure due to increased secretion or decreased outflow of aqueous humor. It is a form of optic neuropathy and causes progressive loss of ganglion cell axons, which may be visualized as a pale optic disc and enlarged optic cup (compared to normal retina). Symptoms evolve over decades, with progressive loss of peripheral visual fields.
Glaucoma is managed with agents that either decrease production or increase outflow of aqueous humor. Latanoprost is a topical prostaglandin used in the treatment of glaucoma. It is applied as a prodrug and converted to the active form by esterases in the cornea. Prostaglandins are the preferred first-line agents for the treatment of glaucoma, and although the exact mechanism of action is uncertain, they have been found to decrease the collagen content in the uveoscleral outflow pathway and increase outflow of aqueous humor. They are also known to cause increased pigmentation in the iris and eyelashes.
(Choices A, C, and E) Carbonic anhydrase inhibitors (eg, dorzolamide) decrease formation of bicarbonate in the ciliary body, leading to decreased sodium and fluid transport and subsequently decreased production of aqueous humor. Alpha-adrenergic agonists (eg, brimonidine) inhibit production of aqueous humor due to vasoconstriction in the ciliary
body. Beta blockers (eg, timolol) also decrease production of aqueous humor. Prostaglandins do not affect production of aqueous humor but are often used in combination with these other agents.
(Choice B) Increased formation of new blood vessels at the optic disc is the characteristic feature of proliferative diabetic retinopathy. Strict control of diabetes will reduce the risk of diabetic retinopathy, but it is not affected by topical prostaglandins.